
Introduction to Social Work: A Look Across the Profession Copyright © 2022 by James Langford, LCSW and Craig Keaton, PhD, LMSW is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, except where otherwise noted.
Mavs Open Press
Arlington
Introduction to Social Work: A Look Across the Profession Copyright © 2022 by James Langford, LCSW and Craig Keaton, PhD, LMSW is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, except where otherwise noted.
1
Creation of this resource was supported by Mavs Open Press, operated by the University of Texas at Arlington Libraries (UTA Libraries). Mavs Open Press offers no-cost services for UTA faculty, staff, and students who wish to openly publish their scholarship. The Libraries’ program provides human and technological resources that empower our communities to publish new open access journals, to convert traditional print journals to open access publications, and to create or adapt open educational resources (OER). Our resources are openly licensed using Creative Commons licenses and are offered in various e-book formats free of charge, which can be downloaded from the Mavs Open Press OER catalog. Optional print copies of this text may be available through the UTA Bookstore or can be purchased directly from XanEdu, Mavs Open Press’ exclusive print provider and distributor.
OER are free teaching and learning materials that are licensed to allow for revision and reuse. They can be fully self-contained textbooks, videos, quizzes, learning modules, and more. OER are distinct from public resources in that they permit others to use, copy, distribute, modify, or reuse the content. The legal permission to modify and customize OER to meet the specific learning objectives of a particular course make them a useful pedagogical tool.
Pressbooks is an open source, web-based authoring tool based on WordPress, and it is the primary tool that Mavs Open Press uses to create and adapt course materials. Pressbooks should not be used with Internet Explorer. The following browsers are best to use with Pressbooks:
Information about open education at UTA is available online. Contact us at oer@uta.edu for other inquires related to UTA Libraries publishing services.
2
Introduction to Social Work: A Look Across the Profession is a collaborative effort among faculty and students in the University of Texas at Arlington School of Social Work. This work is designed to give new social work students and students considering social work a view across the numerous opportunities in the social work profession toward developing their own professional goals and plans.
Introduction to Social Work: A Look Across the Profession was originally developed by then faculty members Jim Langford and Craig Keaton. Later, Regina Praetorius joined the team as editor in the review and revision phase. Regina taught using this text for two semesters. Students in these classes were asked for their honest feedback including ideas for activities, revisions and additions. Emily Clarke, as a BSW student at the time, integrated these revisions and activities into the text. One requested addition was a chapter that focused on working with individuals with disabilities. Emily Clarke and Megan Westmore, a PhD student at the time, took the lead on developing this chapter. Thus, this work is a collaboration across faculty and students toward meeting the needs and interests of students exploring social work as a career. During the Summer of 2023, this book was revised to include updated statistics by PhD student Jessica Williams.
Jim Langford has 35+ years of practicing social work including juvenile probation, hospice, outpatient mental health, and, hospital social work. Prior to my coming to the University of Texas at Arlington School of Social Work as full-time professor, he was a hospital social worker for over 10 years and a hospice social worker for 2 years. He was both a clinical supervisor and direct practitioner with a Fort Worth outpatient mental health agency. His experience as a social work covers a broad range of responsibilities, from management to supervision to direct practice.
3
Creation of this OER was funded by the UTA CARES Grant Program, which is sponsored by UTA Libraries. Under the auspices of UTA’s Coalition for Alternative Resources in Education for Students (CARES), the grant program supports educators interested in practicing open education through the adoption of OER and, when no suitable open resource is available, through the creation of new OER or the adoption of library-licensed or other free content. Additionally, the program promotes innovation in teaching and learning through the exploration of open educational practices, such as collaborating with students to produce educational content of value to a wider community. Information about the grant program and funded projects is available online.
The authors wish to extend gratitude to all the students in Regina’s classes who worked toward making this resource student inspired and student serving.
James Langford, LCSW – Adjunct Professor, University of Texas at Arlington
Craig Keaton, PhD – Texas Christian University
Emily Clarke, BSW, MSW Student – University of Texas at Arlington
Megan Westmore, LMSW, Doctoral Student – University of Texas at Arlington
Regina T. Praetorius, PhD, LMSW-AP, Professor – University of Texas at Arlington
Emily Clarke, BSW, MSW Student – University of Texas at Arlington
Jessica R. Williams, PhD, MSW- University of Texas at Arlington
The authors wish to extend gratitude to all the students in Regina’s classes who worked toward making this resource student inspired and student serving.
1
Learning Objectives
In this chapter the student will be reviewing:
Self-Determination: The priority for social workers to ensure that the client has the information and resources necessary to make an informed decision. Social workers consider this to be an expression of the belief that clients should be treated as experts in their own lives.
Empowerment: The empowerment process is the offering of both knowledge and skills necessary for the target system to achieve the agreed-upon goals. It is based on the notion that role of the social worker is to facilitate change, to be a collaborator in the change process, while carefully avoiding becoming overbearing in the change process.
Strengths-based Approach: Simply put, this is the intent to encourage and develop the strengths of the social worker’s target system, be it the individual, the members of a group, or the community.
Planned Change Process: This is a reference to the process commonly used by social workers. It is a series of steps in the resolving of presenting concerns or problems identified by the target system. The following steps are referred to as the planned change process: engagement, assessment, intervention, and evaluation.
Person-in-Environment: One of the unique features of the social work perspective is the belief that a person must always be consider in the context of their environment. Such a perspective is considered different from a more psychological perspective with its focus on the individual, or sociology with its focus on groups and organizations. Social workers approach the individual from a contextual frame of reference, and such elements of one’s environments would include family, social network (church, community, work), culture, and nation.
What comes to mind when you think of a social worker?
Let me welcome you to an introductory course on a helping profession that includes a Nobel prize urban activist, Jane Addams, and a pioneer writer and researcher on the impact of environment on individuals, Mary Richmond. Both are significant in terms in providing the historical foundation to the profession.
As you might expect from an overview course, time and attention will be given to defining the profession, offering some history on its development into a profession, and professional values and code of ethics. We will review the wide range of roles and responsibilities that are common to the social work practice. Our focus on the practice of social work will include a consideration of what it means to be a generalist practitioner and the 3 modalities of practice: micro, mezzo, and macro. Attention is given to the diverse fields of practice where social workers can be found with major consideration for the more common fields of practice: children and family, mental health and addictions, health, gerontological, administrative, to name a few. We conclude with a look at what might be future opportunities and challenges for new social workers.
The National Association of Social Workers (NASW) has defined the profession of social work in the following way (NASW, 1973, pp 4-5):
Social work is the professional activity of helping individuals, groups, or communities enhance or restore their capacity for social functioning and creating societal conditions favorable to this goal. Social work practice consists of the professional application of social work values, principles, and techniques to one or more of the following ends:
Helping people obtain tangible services (such as housing, food, income)
Providing counseling and psychotherapy with individuals, families, and groups
Helping communities of groups provide or improve social and health services
Participating in relevant legislative process
Another agency overseeing social work education, the Council on Social Work Education (CSWE), states that the purpose of the social work profession is to “promote human and community well-being” Which can be achieved through promoting social and economic justice and preventing conditions that limit human rights for all people. The CSWE’s vision is to ensure a well-educated social work profession equipped to promote health, well-being, and justice for all people in a diverse society.
What do you notice about the definitions of social work? I would like to note a couple of important points. For one, social work is considered a profession, and what qualifies it for such a distinction deserves some attention. Secondly, social work has a dual focus in that it addresses both individual well-being (micro practice) and more systemic well-being (macro practice). We will be addressing both micro and macro practice in this course.
So, what are the characteristics of a social work that qualifies it to be considered a profession?
Let us discuss some of the characteristics of the professional relationship with our clients. They are professional relationships that sets them apart from friendship and family relationships. Such relationships have a recognized purpose, they are time-limited, engage the client in a collaborative manner, they may involve some degree of authority and control, and the relationship is maintained and protected by the professional code of ethics.
Consider the following comparison with other helping professions:
| Disciplines | Similarities | Differences |
|---|---|---|
| Psychology |
|
|
| Health professions |
|
|
| Counseling |
|
|
| Marriage & Family |
|
|
Broker: A common role for social workers linking clients to needed resources.
Case Manager: The coordination of services and resources within an agency or with multiple agencies.
Advocate: Another unique characteristic of the social work profession is the role of advocacy. Such a role relates to one of our core values: social justice. This role is one in which the social work promotes the needs or acts for change on behalf of a client.
Educator: This role is for the social work providing information and the teaching of skills.
Counselor: This is another common role for social workers, and one that can be referred to as a psychotherapist. This role is one in which the social worker facilitates the clients in the identification of problem areas and agreed-upon intervention strategies.
Mediator: The social worker in this role will assist in a dispute resolution process between conflicting parties.
Researcher: Such a social worker role is one of researching programs and policies, and the conducting of studies to improve social service systems.
Group Leader: This social work takes a leadership role for the facilitation of several types of groups, such as task and treatment groups.
Singer, J. B. (Producer). (2014, July 8). #87 – Beginnings, middles, and ends: Stories about social work from Ogden Rogers, Ph.D. [Audio Podcast]. Social Work Podcast. Retrieved from http://socialworkpodcast.blogspot.com/2014/07/ogden.html
Brunner, Allison (2009). When In doubt, give hope.” Social Work Podcast. Retrieved from http://www.socialworkpodcast.com/GraduationSpeech2009.mp3
Singer, J. B. (Producer). (2016, March 28). #103 – The Grand Challenges for Social Work: Interview with Dr. Richard P. Barth [Audio Podcast]. Social Work Podcast. Retrieved from http://www.socialworkpodcast.com/2016/03/grand-challenges.html
American Academy of Social Work and Social Welfare. (2017). Grand challenges for social work. Retrieved from https://grandchallengesforsocialwork.org/
Asquith, S., Clark, C. L., & Waterhouse, L. (2005). The role of the social worker in the 21st century: A literature review. Edinburgh: Scottish Executive Education Department.
Bent-Goodley, T.B. (2017). Readying the profession for changing times. Social Work, 62(2), 101-103. https://academic.oup.com/sw/article/62/2/101/3044152
Blundo, R. (2001). Learning strengths-based practice: Challenging our personal and professional frames. Families in Society: The Journal of Contemporary Social Services, 82(3), 296-304. https://journals.sagepub.com/doi/pdf/10.1606/1044-3894.192
Brown, B. (December. 2013). Brené Brown on empathy. Retrieved from https://www.youtube.com/watch?v=1Evwgu369Jw&feature=youtu.be
Brunner, A. (2009) When in doubt, give hope [Audio file]. Social Work Podcast. Retrieved from http://www.socialworkpodcast.com/GraduationSpeech2009.mp3
Clark, E. J. (2017). 10 essentials social workers must know about hope [Blog post]. Retrieved from http://www.socialworker.com/feature-articles/practice/10-essentials-social-workers-must-know-about-hope/
Clark, E. J., & Hoffler, E. F. (2014). Hope matters: The power of social work. Washington, DC: NASW Press.
Corey, M., Corey, G., & Corey, C. (2014). Groups: Process and Practice (9th ed.) Pacific Grove, CA: Brooks/Cengage Learning.
Council on Social Work Education (CSWE), Commission on Accreditation. (2016, July). Handbook of social work accreditation policies and procedures. Retrieved from https://cswe.org/Accreditation/Standards-and-Policies/EPAS-Handbook
D’Aprix, A. S., Dunlap, K. M., Abel, E., & Edwards, R. L. (2004). Goodness of fit: Career goals of MSW students and the aims of the social work profession in the United States. Social Work Education, 23(3), 265-280. http://dx.doi.org/10.1080/0261547042000224029
Gibelman, Margaret. (1999). The search for identity: defining social work – past, present, future. Social Work, 44(4) p298-310. doi: 10.1093/sw/44.4.298
Grinnell, R.M., & Unrau, Y.A. (2010). Social work research and evaluation: Foundations of evidence-based practice [9th ed.]. New York: Oxford University Press.
Hunter, R. (1904). Poverty. New York: The Macmillan Company. Retrieved from https://archive.org/details/povertypoor00huntuoft
Jane M. Hoey (1892-1968): Social worker, welfare administrator, government official. (2011). In Social Welfare History Project. Retrieved from http://socialwelfare.library.vcu.edu/people/hoey-jane-m/
Kerson, T. S., & McCoyd, J. (2013). In response to need: An analysis of social work roles over time. Social Work. 58(4) 333-343. doi: 10.1093/sw/swt035
Langer, C. L., & Lietz, C. (2014). Applying theory to generalist social work practice. Hoboken, NJ: Wiley.
McLaughlin, H. (2008). What’s in a name: ‘Client,’ ‘patient,’ ‘customer,’ ‘consumer,’ ‘expert by experience,’ ‘service user’—What’s next? British Journal of Social Work, 39(6), 1101-1117. https://doi.org/10.1093/bjsw/bcm155
National Association of Social Workers (NASW). (2021). Code of Ethics of the National Association of Social Workers. Washington, DC: NASW Press. Retrieved from https://www.socialworkers.org/About/Ethics/Code-of-Ethics/Code-of-Ethics-English
Rothman, J., & Mizrahi, T. (2014). Balancing micro and macro practice: A challenge for social work. Social Work, 59(1), 91-93.
Sheafor, B. W., Horejsi, C. R., & Horejsi, G. A. (2000). Techniques and guidelines for social work practice (5th ed.). Boston: Allyn and Bacon
Singer, J. B. (Producer). (2014). #87 – Beginnings, middles, and ends: Stories about social work from Ogden Rogers, Ph.D. [Audio podcast]. Social Work Podcast. Retrieved from http://socialworkpodcast.blogspot.com/2014/07/ogden.html
Singer, J. B. (Producer). (2016). #103 – The Grand Challenges for Social Work: Interview with Dr. Richard P. Barth [Audio podcast]. Social Work Podcast. Retrieved from http://socialworkpodcast.blogspot.com/2016/03/grand-challenges.html
Social Work Degree Guide. (2017). Five differences between BSW and MSW programs. Retrieved from http://www.socialworkdegreeguide.com/lists/five-differences-between-bsw-and-msw-programs/
Stoesen, L. (2006). Mediation a natural for social workers. NASW News, (51)8.
Uehara, E.S., Barth, R. P., Olson, S., Catalano, R. F., Hawkins, J. D., … Sherraden, M. (2015). Identifying and tackling grand challenges for social work. (Grand Challenges for Social Work Initiative, Working Paper No. 3). Retrieved http://aaswsw.org/wp-content/uploads/2015/12/WP3-with-cover.pdf
Zastrow, C. (2016). Generalist social work practice: A Worktext (11th ed). Chicago: Lyceum Books, Inc.
2
“The focus for practice in a helping profession is faith in the possibilities within people, if given the right conditions for growth.”
– Social Worker Bertha Capen Reynolds (1885-1978)
A timeline of all the historical milestones
https://online.simmons.edu/blog/evolution-social-work-historical-milestones/
The inception of the social work profession in the United States can be traced back to the late nineteenth century beginning with charity work performed by local churches and communities hoping to meet the needs of the poor. Some of the earliest social work interventions were designed to meet basic human needs of populations and placed great value in providing support, assistance, and resources to families and communities to alleviate suffering (Nsonwu, Casey, Cook & Armendariz, 2013). This was the beginning of the progressive movement era. Many progressive-minded individuals began to speak out about social injustices during the rise of the industrial revolution. Many major cities wanted to attract business, so taxation was kept to a minimum. This left little or no money to provide social services for the poor. This lack of protections for the most vulnerable Americans caused progressives to criticize the lack of government intervention and involvement in social welfare (Flanagan, 2007).
The settlement house movement called for a social reformation of America. The plight of the poor called many to the movement and ushered in the helping hands of early social workers (Flanagan, 2007). Stanton Coit founded the first settlement house, University Settlement, in New York City’s lower east side in 1886 after he toured settlement houses of England (Trolander, 1991). Jane Addams, an educated upper middle-class woman from Illinois, founded Hull-House in 1889 in Chicago. Hull-House was a successful settlement house located in an area that was largely populated by poor working immigrants. Residents of Hull-House were provided with multiple services including daycare and kindergarten for children, a library, art classes, adult literacy courses, music, and various other facilities (Paul, 2016). When Addams was a young woman, after she finished college, she traveled to London and visited Toynbee Hall settlement house. She was inspired to return home and start a similar organization where she could employ the same social services she observed at Toynbee Hall. Although Hull-House was not the first settlement house in America, it became the most well-known (Trolander, 1991). Jane Addams would go on to be an activist in the anti-child labor movement where she advocated for the rights of child workers. This activism would eventually assist in the passage of the Child Labor Law in 1916. In 1931 Addams would be awarded the Nobel Peace Prize for her continued commitment to social justice and reform (Paul, 2016).
For much more on the life and work of Jane Addams, see the video link at the beginning of this section. Final note as you look forward to more recent movements in social work and social justice, it was noted in a comment for the video that “Even though Addams was willing to offer Teddy’s (Theodore Roosevelt) nomination at the Progressives Convention, she was angry about his lack of inclusion of [people of color] …and consequently was a primary fundraiser for the founding of the NAACP.”

Mary Richmond was born in Illinois in 1861, but she was raised by her grandmother in Baltimore Maryland after her parents died at a young age. She was raised learning about social, political, and cultural issues of the time (Social Welfare History Project, 2011). After she graduated high school, she went to work as a bookkeeper for several years as she did not have the opportunity to attend college. She eventually applied for a position with the Charity Organization Society, (COS) in 1889. The Charity Organization Societies in several cities were the first organizations to develop a structured social work profession, providing social services to the poor, disabled, and needy. During the time Richmond was connected to the COS, she demonstrated her qualities as a leader, teacher, and practical theorist. Richmond’s ability to explain the mission and purpose of the organization as well as raise money to support the services that the organization provided, resulted in her being appointed as the first woman general secretary of the COS (Social Welfare History Project, 2011).
Mary Richmond’s lasting impact on the field of social work comes from her commitment to ensuring families receive appropriate services. Richmond sought to fully understand the problems of the poor and worked to train her staff to assist families in a structured manner. She felt that professionalization of social service would mean that poor families would receive better treatment and therefore improve their circumstances (Social Welfare History Project, 2011). One of Richmond’s biggest contributions to the social work profession was her book Social Diagnosis which was published in 1917. Richmond’s book focused on the practice of casework with individuals and was the first book to identify a systematic and methodological way to document and diagnose clients (Social Welfare History Project, 2011). Richmond states in her book, when people are sick, we can cure them; when they are bad, we can try to reform them but when they are out of work there is only one effective remedy for their troubles and that is real work at real wages. (Richmond, 1922, p. 208)

The practice and profession of social work was heavily involved in the Great Depression programs of the New Deal put forth by President Roosevelt (Leighninger, 2019). Mary Richmond’s model that included social reform as an essential part of social work was used by caseworkers in developing programs to assist families. Public works programs developed as part of the New Deal helped people in many ways. The earliest programs provided out of work individuals with a job and steady income (Leighninger, 2019).
Several professional social workers played vital roles in the development of New Deal programs to assist the American public during the Great Depression. Jane Hoey’s career as a social worker began in 1916 when she was appointed as the Assistant Secretary of the Board of Child Welfare in New York City. Hoey is best known for her role in the enactment of the Social Security Public Assistance Act which became law in 1935. Following the law’s enactment, Hoey became the Director of the Bureau of Public Assistance within the Social Security Administration and was responsible for organizing and implementing the distribution of the public welfare provisions (Social Welfare History Project, 2011).
Harry Hopkins became the Federal Relief Administrator during the Great Depression and presidential advisor. Hopkins believed that the way to assist people during a time of such job loss was to get people back to work instead of direct government handouts. Hopkins led such New Deal programs as the Federal Emergency Relief Administration (FERA), the Civil Works Administration (CWA), and the Works Progress Administration (WPA) (Hopkins, 2011). These programs not only helped to create work and income for struggling families, but they also helped with morale which Hopkins and other social workers of the time deemed necessary (Leighninger, 2019).
https://www.youtube.com/watch?v=a4VzRSnksmA
Legacies of Social Change from CSWE and NASW on Youtube.
The evolution of Social Work: Historical milestones. SC-UMT. (2021, May 13). Retrieved April 17, 2022, from https://online.simmons.edu/blog/evolution-social-work-historical-milestones/
Hansan, J.E. (2013). Hunter, (Wiles) Robert (April 10, 1874 – May 15, 1942), social worker, author and socialist. In Social Welfare History Project. Retrieved from http://socialwelfare.library.vcu.edu/people/hunter-robert/
Leighninger, R. (2019). Families, The Family, and the New Deal. Families in Society: The Journal of Contemporary Social Services. 100(4) 341–350. https://doi.org/10.1177/1044389419874904
Nsonwu, M. B., Casey, K., Cook, S. W., & Armendariz, N. B. (2013). Embodying social work as a profession: A pedagogy for practice. SAGE Open, 3(3), 1-8. https://doi.org/10.1177/2158244013503835
Paul, C.A. (2016). Jane Addams (1860-1935). Social Welfare History Project. Retrieved from http://socialwelfare.library.vcu.edu/settlement-houses/addams-jane/
Richmond, M. E. (1917). Social diagnosis. New York: Russell Sage Foundation
Social Welfare History Project (2011). Mary Ellen Richmond (1861-1928) – Social work pioneer, administrator, researcher, and author. Social Welfare History Project. Retrieved from http://socialwelfare.library.vcu.edu/social-work/richmond-mary/
Trolander, J.A. (1991). Hull-House and the settlement house movement: A centennial reassessment. Journal of Urban History, 17(4), 410-420. https://journals.sagepub.com/doi/pdf/10.1177/009614429101700404
3
Social work is considered a helping profession. Like many other helping professions such as nursing, counselling, teaching, and psychiatry, social work has ethical guidelines to help direct and guide the work (Cournoyer, 2011). Helping professions address a multitude of problems or dilemmas often involving a person’s physical, mental, social, intellectual, and spiritual well-being. Therefore, social workers are responsible for many important decisions. Often these decisions involve ethical choices in the best interest of clients’ lives. These decisions can be extremely difficult and emotionally charged and may not always be the choices the professional is comfortable making.
The purpose of this chapter is to provide a brief understanding of the NASW Code of Ethics as you begin your journey into the foundations and practice of social work. This chapter is designed to explore and help provide a base understanding of the terms and overall principles related to social work ethics and professional practice. Finally, for those pursuing a social work degree, the goal is to prepare you for future courses and your future career, so you are familiar with the general concepts, as you will continue to explore and apply the NASW Code of Ethics throughout your education. (Keywords: ethics, values, obligations, and duties)
As social work endeavored to gain recognition as a profession, the need arose for a formal code of ethics. While there were many social workers who helped pave the way, Mary Richmond is considered one of the most important. In 1920, Mary Richmond provided an experimental Code of Ethics which served as a base for many other social workers seeking justice, equality, and fairness for vulnerable and oppressed populations (Reamer, 2006). Richmond’s Code of Ethics served as a guide to the first edition of the NASW Code of Ethics which was constructed in October of 1960. This document, developed by the NASW’s Delegate Assembly of the National Association of Social Workers, officially defined the duties and obligations for which a social worker is responsible. The 1960 edition defined fourteen responsibilities social workers were obligated to fulfil based on the mission of social work, and even included a discrimination clause. With the first revision in place, the social work profession established a sense of professionalism. Over the years, major revisions have taken place:
Provided is a link with all updated changes: https://www.socialworkers.org/LinkClick.aspx?fileticket=UyXb_VQ35QA%3D&portalid=0#:~:text=After%20careful%20deliberation%20via%20the,Competence%E2%80%9D%20as%20it%20relates%20to
We have the code of ethics in place to:
The NASW Code of Ethics consists of four sections (Woodcock, 2011):
The preamble is intended to outline Social Work’s mission and core values. Social Work’s mission is “to enhance human well-being and help meet the basic human needs of all people, with attention to the needs and empowerment of people who are vulnerable, oppressed, and living in poverty” (Cournoyer, 2011, p. 160). With this mission, social workers have a clear indication of what is expected when entering the field and practicing as a social worker. Every agency and organization will have their own guidelines and rules, and it is then the social worker’s responsibility to incorporate those guidelines along with the NASW Code of Ethics. Social workers have many distinct roles and can be found in many areas of work, with the primary goal always to endorse social justice (Woodcock, 2011).
The purpose of the NASW Code of Ethics is to hold social workers to a high standard of professionalism. The NASW Code of Ethics serves six purposes (NASW, 2008):
The NASW Code of Ethics cannot guarantee that it covers all ethical behaviors. There may be times when social workers will not be sure what to do or what decision to make, which then leads to frustration. The Code of Ethics is intended to guide the process of difficult decision making to come to the best conclusion. Working closely with a supervisor is also an important part of the process. It is up to the social worker to become familiar with and follow the Code of Ethics and best represent the profession.
The ethical principles are based on the six core values of social work. These six values are important for all social workers to recognize and apply to their practice. They should help direct all ethical decisions or dilemmas encountered. Social workers should also be conscientious of these values when working with clients, talking with co- workers, writing grants, or any other role a social worker performs, even if an ethical dilemma does not present itself.
The six core values of social work are:
(Reamer, 2006).
The ethical standards of social work consist of six important criteria for which all social workers are held responsible. These are social workers’ ethical responsibilities:
Common ethical violations to be aware of consist of the following:
(Cournoyer, 2011)
In summary, the NASW Code of Ethics is a living document and will continue to be adjusted as new developments and issues arise. The Code also enforces the belief that the public will not be taken advantage of by the work of social workers for their own benefit and that clients will be treated fairly. Therefore, social workers are responsible for staying updated on all changes that are made and applying them in practice.
Another critical aspect of ethical social work is the legal obligations and responsibilities. These duties are profoundly serious, and all social workers must abide by them. These duties or obligations consist of:
An important term in this chapter is confidentiality. The term confidentiality indicates that any information shared by a client or pertaining to a client will not be shared with third parties (Cournoyer, 2011). Confidentiality is extremely important for social workers as they have a duty to keep client information and conversations between the social worker and the client. Social workers should not only protect the information gained from clients, but they should also respect information shared by colleagues. If confidentiality is broken, it can be a serious violation. An important confidentiality law is the U.S. Health Insurance Portability and Accountability Act (HIPAA) which is commonly found in the health profession. HIPAA assures that client information will remain private between client and professional.
There are times when a social worker is required to break the confidentiality rule. This is known as duty to report. Social workers are mandated reporters and have a legal obligation to report to the designated authority if a client disclosed any of the following (Cournoyer, 2011):
These circumstances are the only time that a social worker is legally obligated to breach confidentiality agreements and must be taken very seriously.
Social workers are required to educate clients concerning the scope of the services. This consists of informing the client about the role of the social worker, confidentiality, duty to report, the cost, length of treatment, risks, alternative services, and anything else the agency requires (Cournoyer, 2011). This process is often completed early, when the first meeting with a client or in advance of the first meeting. Not informing a client of the social worker’s roles, responsibilities, and obligations can be a form of malpractice, which is discussed later in the chapter.
Privacy differs from confidentiality because it refers to the client’s right to choose what to share and what to not share with a social worker. Social workers must respect that there may be things the client does not wish to disclose and cannot be forced to do so. It is a social worker’s duty to respect the relationship they have with clients and to not intrude on their lives outside of their sessions. For example, if a social worker is working in a small town and runs into a client at the grocery store, it is in the best interest of the social worker and client to respect the privacy of that individual and not approach them. Nor should a social worker discuss what was previously talked about during a client session together. Social workers should discuss these possibilities with their clients so they are aware of how they will react to their clients if they meet in a public setting.
Along with many other helping professions, a social worker is obligated to act to ensure that anybody who may be in danger is aware of the possible danger. Social workers have the responsibility to warn potential victims that a client may harm them (Cournoyer, 2011). Therefore, social workers must take serious action in deciding if a client is serious about harming another person. A case to be familiar with is the well-known Tarasoff v. Regents of the University of California in which the Supreme Court ruled that mental health professionals have a duty to protect individuals of a third party who may be threatened or harmed by a client, in which now is known as duty to warn and protect (Dolgoff, Harrington, & Loewenberg, 2009).
Situations where there is no clear answer, being required to choose between two or more decisions, or being faced with contradictory decisions with often undesirable outcomes for one or more persons (Dolgoff, Harrington, & Loewenberg, 2009) are examples of ethical dilemmas.
Ethical dilemmas are often known as the grey area of social work. Therefore, social workers must know themselves very well, be conscious of the Code of Ethics, and let the Code guide them to making these decisions. Some common ethical dilemmas include:
There are many tips and suggestions for ethical problem solving, Dolgoff, Harrington, & Lowewenberg (2009) suggest considering the following when making ethical decisions:
Often social workers are alone when they must make difficult choices and cannot always seek supervision right away. Therefore, social workers must be prepared to handle these situations on their own. The ETHIC Model of Decision Making may be helpful (Cournoyer, 2011; Congress, 2000, p. 10):
E – Examine relevant personal, societal, agency, client, and professional values
T—Think what ethical standard of NASW Code applies, and relevant laws and case decisions
H—Hypothesize about consequences of different decisions
I—Identify who will benefit and who will be harmed
C—Consult with supervisor and colleagues about the most ethical choice
Malpractice can be defined as a form of negligence which occurs when a licensed social worker is not consistent with the professions’ Code of Ethics, standards of care, and is negligent to his or her legal duties and obligations (Reamer, 2006). Often this involves poor delivery of services or a social worker failing to meet the standard of care at his or her agency. Three common forms of malpractice include:
(Cournoyer, 2011)
Malpractice can occur even if one intentionally or unintentionally is aware of the wrongdoing. For example, a genuine mistake social workers make is simply forgetting to obtain a client’s consent before sharing confidential records with third parties. This alone can lead to serious civil lawsuits and can jeopardize your social work license. When these mistakes occur, the social worker does not intend to cause harm, but due to the many responsibilities social workers have it is easy to forget and unintentionally make this mistake (Reamer, 2006). Some common examples of malpractice include the following (Reamer, 2006; Cournoyer, 2011):
It is important for practicing social workers to have insurance coverage to protect in case of a lawsuit. Social workers will often be covered by their agency, and the NASW also provides legal coverage to social workers.
The NASW Code of Ethics does not list any value or ethic as more important than the next. Therefore, one must consider all professional values and ethics as equal. To be a professional social worker, one should be well acquainted with the Social Work Code of Ethics along with the six core values. Furthermore, ethical decision-making takes skill and practice, and is a never-ending process (Reamer, 2006). If pursuing a career in Social Work, the more you prepare yourself, know yourself, and follow the Code of Ethics, the greater skill you will obtain as a professional social worker (Cournoyer, 2011). Finally, the Code of Ethics and 6 Core Values originated from the idea that all people are equal and deserving of the same entitlements. Social workers, through the Code and Core Values, share responsibility for continuing and promoting social justice.
Congress, E. P. (2000). What social workers should know about ethics: Understanding and resolving ethical dilemmas. Advances in Social Work, 1(1), 1-25.
Cournoyer, B. (2011). The social work skills workbook (7th ed.). Belmont, CA: Brooks/Cole.
Dolgoff, R., Harrington, D., & Loewenberg, F. M. (2009). Ethical decisions for social work practice (9th ed.). Belmont, CA: Brooks/Cole
Morales, A. T.., Sheafor, B. W., & Scott, M. E. (2010). Social work: A profession of many faces. New York: Pearson Custom Publishing.
National Association of Social Workers. (2021). NASW Code of Ethics. Retrieved from https://www.socialworkers.org/About/Ethics/Code-of-Ethics/Code-of-Ethics-English
Reamer, F. G. (2006). Social work values and ethics (2nd ed.). New York, NY: Columbia University Press.
Woodcock, R. (2011). Ethical standards in the NASW code of ethics: The explicit legal model and beyond. Families in Society, 92(1), 21-27. doi.org/10.1606/1044-3894.4052
4
Learning Objectives
In this chapter, the student will be reviewing the following:
If ever there was a moment in our society that we need to be exploring such topics as culture, race, ethnicity, and diversity, that time would be now. We are witnessing in our national discourse an outpouring of public demonstrations following several recorded acts of police brutality. Not since the 1960s has there been such large- scale marches throughout this nation as well as in major cities throughout the world. Triggered by the recorded acts of police violence on African Americans has expanded into a national discussion on the history of race in this country. This chapter will be a consideration of race, culture, diversity, along with a discussion of several at-risk populations.
Let us begin with a discussion of culture. What is culture? Many individuals think of culture as something that is different from them. They may think of culture as something they desire to have; they mistakenly do not realize that everyone has culture. Culture is something that all of us have but because we live it, we do not realize that it is there. When we think of culture, we think of many ways of life for others; we often neglect to understand that what we do in our everyday lives is different than others. We simply think of our lifestyles as “normal,” not cultured.
Garthwait, MSW (2012) as: customs, beliefs, ideology, worldview, and values common to a group of people and which guide their individual and social behavior. More specifically, it is the product of the values, ideas, perceptions, and meanings which have evolved over time. These values, ideas, perceptions, and meanings constitute the individual’s knowledge and understanding of the world in which he or she lives.
They derive from:
Stated simply, race is the word used to describe the physical characteristics of a person. These characteristics can include everything from skin color, eye color, facial structure, or hair color. This term is physiological in nature and refers to distinct populations within the larger species. Race was once a common scientific field of study. Today, however, most scientists agree that genetic differences among races do not exist which means we are all the same inside. Clearly, we all have the same make-up which consists of vitamins, minerals, water, and oxygen.
What are your thoughts on this consideration of race that pertains to the many varied physical variations for humankind, but that “we are all the same inside?”
Ethnicity denotes groups, such as Irish, Fijian, or Sioux, for example, that share a common identity-based ancestry, language, or culture. It is often based on religion, beliefs, and customs as well as memories of migration or colonization (Cornell & Hartmann, 2007).
Ethnicity, on the other hand, is the word used to describe the cultural identity of a person. These identities can include language, religion, nationality, ancestry, dress, and customs. The members of a particular ethnicity tend to identify with each other based on these shared cultural traits.
What is the difference between race and ethnicity?
Race is identified through biology and described by physical characteristics such as skin color. Ethnicity is cultural expression and identification. (Blakemore, 2019)
A Cultural Questionnaire
Take a moment to reflect on each of the following. How do these look for you? What aspects are important to you? How does your family engage with each of these? What about people in your neighborhood? How might it differ for someone of a different cultural background?
Cultural expressiveness: dress, food, music, arts, holidays: ____
Beliefs about education: ____
Beliefs about family, family structure, kinship bonds: ____
Beliefs about children & child rearing: ____
Partnering: ____
Gender roles: traditional vs. more modern gender roles: ____
Social values, sense of community: ____
Religion & Spirituality: ____
Help-seeking behavior: use of indigenous & traditional healing practices: belief about the dying process (advanced directives, post death practices): ____
It is important for social workers to understand the concept of culture in order to have cultural competence. This can be defined as a set of behaviors, attitudes, and policies that come together in a system, agency, or program. It can also be among individuals, enabling them to function effectively in diverse cultural interactions and similarities within, among, and between groups. Another way to describe cultural competence is a point on a continuum that represents the policies and practices of an organization, or the values and behavior of an individual which enable that organization or person to interact effectively in a culturally diverse environment. The competency of social workers is limited when they do not possess tools of acknowledgment that can affect them when working with diverse populations.
NASW Code of Ethics on cultural competency: Standard 1.05(c): “to obtain education about and seek to understand the nature of social diversity and oppression.” NASW’s National Committee on Racial and Ethnic Diversity (NASW, 2001) highlights this necessity by identifying standards that make up culturally competent practices, including self-awareness, cross-cultural knowledge, skills, and leadership.
Social workers must possess the skills to be able to understand a broad spectrum of varying cultures and understand important and influential beliefs related to that specific culture. An informed social worker will better understand how culture and diversity may impact, how we present services and treatment and what interventions could produce better outcomes for those we serve. It would be useful for a social worker to be bilingual but not required as most agencies have access to interpreters.
A Cultural Competency Activity:
McIntosh (1989) further describes white privilege as an “invisible package of unearned assets, which one can count on each day. White privilege is like an invisible weightless knapsack of special provisions, maps, passports, code books, visas, clothes, tools, and blank checks.”
McIntosh’ White Privilege Checklist: http://also-chicago.org/also_site/wp-content/uploads/2017/03/white-privilege.pdf
Recognition of lesbian, gay, bisexual, and transgender people as a minority group or groups has gained prominence in Western culture since the nineteenth century. The abbreviation “LGBTQ” is currently used to group these identities together. The term queer is sometimes understood as an umbrella term for all non-normative sexualities and gender expressions but does not always signify a minority; rather, as with many gay rights activists of the 1960s and 1970s, it sometimes represents an attempt to highlight sexual diversity in everyone.
There is a growing realization that sexual and gender groups face discrimination, violence, and criminalization. For example, nearly eighty countries criminalize homosexuality in some way (Park, 2016). Cultural stigma prohibits sexual and gender groups from reaching their full potential. Stigma is an attribute, or mark on, another person. In the context of social interaction, it is a shared belief about someone’s characteristics and traits.
Diverse gender identity groups can be identified and grouped according to any one of the three different categories:
Diverse sexual orientation groups can be identified and grouped according to:
Persons belonging to diverse religious groups have a faith which is different from that held by the majority population or the population group that is in power. It is now accepted in many multicultural societies around the world that people should have the freedom to choose their own religion as well as including not having any religion (atheism or agnosticism) and including the right to convert from one religion to another. However, in some countries, this freedom is still either formally restricted or subject to cultural bias from the majority population.
The disability rights movement has contributed to an understanding of people with disabilities as a minority or a coalition of minorities who are disadvantaged by society, not just as people who are disadvantaged by their impairments. Advocates of disability rights emphasize differences in physical or psychological functioning rather than inferiority: for example, some people with autism argue for acceptance of neurodiversity in the same way opponents of racism argue for acceptance of ethnic diversity. The deaf community is often regarded as a linguistic and cultural minority rather than a group with disabilities, and some deaf people do not see themselves as having a disability at all. Rather, they are disadvantaged by technologies and social institutions that are designed to cater to the dominant, hearing-unimpaired group.
Immigration involves the permanent movement from one country to another. Social workers are often called upon to work with immigrants. Immigrants represent a significant portion of the U.S. population. In 2020, 13.6% of the total population were foreign-born (U.S. Census Bureau, n.d.).
People with different national origins often find it difficult to integrate into mainstream culture, especially when language barriers exist, or they experience immigration issues. Social workers play a crucial role in many immigration cases. A social worker is often the first-person people talk to about their immigration struggles. Social workers often help clients gather key evidence, write detailed evaluations, assist with citizenship, or change of legal status, or are the primary contact with police officers. There is a range of immigration status which immigrant children, youth and parents may hold. Immigrants may fall into one of the following categories:
ESource: NASW Quick Resource Guide, 2013
Based on the notion that effective social work practice must include an understanding and appreciation of diversity, the following section provides such information. The following section discusses some of the values, beliefs, and perspectives assumed by several cultural groups in our society: African Americans, Hispanic/Latinx, Indigenous and Tribal Americans, Asian Americans, and Muslim Americans.
As of the 2020 census, there are about 41.1 million Black or African American people in the United States (U.S. Census Bureau, n.d.). African Americans, like other racial, cultural, and ethnic groups, reflect great diversity.
Common themes: importance of extended family, role flexibility, high respect for older adults, and strong religious beliefs and a close relationship with the church.
For more information on African Americans: African Americans in U.S. History in Context
Hispanic American Heritage
As we know, no one term is acceptable to all groups of people. Hispanic and Latino/Latina have generally been used to refer to people originating in countries in which Spanish is spoken. However, we have also established that the terms refer to people originating in a wide range of places. Others prefer to be addressed by their specific countries of origin. For example, people from Puerto Rico prefer to be addressed as Puerto Ricans. In 2020, there are about 62 million Hispanic or Latino people in the United States (U.S Census Bureau, n.d.). The largest Hispanic orgin group in the US are Mexican, making up nearly 60% of all Hispanic Americans. Other large groups include Puerto Rican, Slavadorian, Cuban, and Dominaican (Krogstatd et al., 2022). It is important not to make stereotyped assumptions about such a diverse group.
Common themes: The first theme important in understanding the environment for children growing up in Hispanic families is the significance of a common language. A second theme reflecting a major strength in many Hispanic families is the significance placed on relationships with nuclear and extended family, including aunts, uncles, cousins, and grandparents, as well as close friends. A third theme characterizing many Hispanic families is the importance of spirituality and religion. Catholicism is a defining role for family and gender roles for Latino or Hispanic people. A fourth theme often characterizing Hispanic families is the strict gender roles.
For more information on Hispanic Americans: http://www.dimensionsofculture.com/2011/03/cultural-values-of-latino-patients-and-families/
In the United States, there are about 700 native groups (Indian and Eskimo) that still exist. Of that number, about 556, including some 223 village groups in Alaska, are formally recognized. (For a listing of federally recognized groups, log on to https://www.ncai.org/about-tribes) (Sutton, 2004).
Each Native American group has always had a name for itself – a name that often translates to something like “The People.” However, groups have often been known to the outside world by other names (i.e., American Indian, Native American, and First Nation’s Peoples) (Weaver, 2008). Whenever possible, it is best to identify the participants’ specific group. As part of their increasing pride and power, many groups are trying to revive their original names and asking that these be used instead of other names. For example, the Chippewa, Ottawa, and Potawatomi want to be called Anishinaabe (“The People from Above”).
Common themes: Several themes characterize many Native American people. These include the importance of extended family and respect for older adults, noninterference, harmony with nature, the concept of time, and spirituality.
For more information on Native Americans: http://pluralism.org/religions/native-american-traditions/
There are nearly 20 million Asian people in the US at the time of the 2020 Census (U.S., Census Bureau, n.d.) and represented more than thirty different nationalities and ethnic groups, including Samoan, Tongan, Guamanian, and native Hawaiian from the Pacific Islands; Lao, Hmong, Mien, Vietnamese, Cambodian, Thai, Burmese, Malay, and Filipinos from Southeast Asia; Pakistani, Bangladeshi, Indian, and Sri Lankan from South Asia; Afghani and Iranian from Central Asia; and Korean, Japanese, and Chinese from East Asia. In 2019, the three largest Asian nationalities in the United States were Chinese, Indian, and Philipino (Budiman & Ruiz, 2021). The diversity of Asian Americans, in terms of their various languages, cultures, and histories, is remarkable (Kiang, 2017). Obviously, there is a huge variation among these groups despite the fact that they are clustered under the same umbrella term Asian Americans.
Common themes: Four themes tend to be similar throughout the diverse groups. These include family as the primary unit and individuality as secondary in importance, interdependence among family, filial piety, and their involvement in patriarchal hierarchy.
For more information on Asian Americans: http://www.asian-nation.org
Since the U.S. Census Bureau does not ask questions about religion, there is no official government count of the U.S. Muslim population. It has been estimated, by Pew Research, in 2015 that there were 3.3 million Muslims of all ages in the United States. Islam is the second largest religion in the world and third largest in the United States (Lipka, 2017). As a social worker, it is likely that you will work with an individual who identifies as a Muslim.
It is important to understand that, unlike the previous cultures discussed, we are attempting to give a brief overview of the religion Islam and not the people. Like any religious group, religious beliefs and practices of Muslims vary depending on many factors including where they live. Each of these cultures’ practices Islam to a different degree just as many Christians practice their religion at different degrees. For example, a Muslim individual from Saudi Arabia may be extremely strict with the way that women should dress while an individual from Turkey may be more relaxed.
Common themes: Social values are divided into three groups: necessities (dharuriyyat); convenience (hajiat); and refinements (kamaliat). Human basic values consist of life (al nafs), reason (al’aql), descent (nasab), property (al mal) and religion (al din) (Akunduz, 2002). Islam protects these primary human values and prohibits any violation of them.
For a brief introduction to Islam go to: http://www.islamicity.com/mosque/Intro_Islam.htm
For more information on Muslim Americans: https://www.cfr.org/backgrounder/muslims-united-states
Being culturally competent and having cross-cultural awareness is an ongoing process. It clarifies the circumstances and social issues from a client’s perspective. Competency is also important as social workers must attend to their own perspectives about their own cultural identity and how the client may view us. The need to assess all aspects of a client’s belief system, values, and how they view themselves within their own culture is as important as assessing their whole bio- psychosocial history. By having some understanding of and sensitivity to other cultures means that we can also help others learn about different views and perspectives. Most importantly, we can dispel any generalizations or myths about a certain culture. With better insight we can appropriately match clients’ needs in respect to resources and services.
Related to one of the unique roles for social workers, being an advocate, cultural competency is about being the voice of our client(s) whether it is for an individual, a group, a neighborhood, or organization, in order to make sure that their rights are not violated, and they are treated with dignity and respect. Learning to deal with how and what types of social issues regarding injustices exist will help when we are dealing with real life discrimination and inequality that occurs and may be affecting our clients. By understanding and identifying social injustice and inequality, we can offset mechanisms of oppression and how they work.
In summary, social workers must possess the skills to be able to understand a broad spectrum of varying cultures and have an understanding of important and influential beliefs related to that specific culture. An informed social worker will better understand how culture and diversity impacts our clients and we can more effectively provide the necessary services and treatment.
Akunduz, A. (n.d.). Norms and values in Islam. Rotterdam: Islamic University of Rotterdam. Retrieved from http://islam.uga.edu/norms_values.html
Allport, G. (1979). The nature of prejudice (25th ed.). Reading, MA: Addison-Wesley.
Bala, N. (n.d.). Islam: Information of the great world religion, its people and their way of life. Retrieved from http://www.greenstar.org/Islam/
Barbarin, O. A. (1983). Coping with ecological transitions by Black families: A psycho- social model. Journal of Community Psychology, 11(4):308–322.
Blakemore, E. (2021, May 3). Race and ethnicity facts and information. Culture. Retrieved February 13, 2022, from https://www.nationalgeographic.com/culture/article/race-ethnicity#:~:text=%E2%80%9CRace%E2%80%9D%20is%20usually%20associated%20with,and%20characterize%20seemingly%20distinct%20populations.
Budiman, A., & Ruiz, N. G. (2021). Key facts about Asian origin groups in the U.S. Retrieved from https://www.pewresearch.org/short-reads/2021/04/29/key-facts-about-asian-origin-groups-in-the-u-s/
Capps, R. & Passel, J. S. (2004). Describing immigrant communities. In Foundation for Child Development. Retrieved from https://www.fcd-us.org/assets/2016/04/DescribingImmigrantCommunitites.pdf
Cornell, S., & Hartmann, D. (2007). Ethnicity and race: Making identities in a changing world. Thousand Oaks, CA: Pine Forge Press.
Cosmides, L., Tooby, J., & Kurzban, R. (2003). Perceptions of race. TRENDS in Cognitive Science, 4(7), 173-179.
Damen, L. (1987). Culture learning: The fifth dimension on the language classroom. Reading, MA: Addison-Wesley.
Duster, T. (2009). Debating reality and relevance. Science, 324(5931), 1144-1145. doi: 10.1126/science.1174523
Fadiman, A. (1997). The spirit catches you and you fall down. New York: Farrar, Straus and Giroux.
Garthwait, C. (2012, October). Dictionary of social work. Missoula: The University of Montana. Retrieved from https://www.umt.edu/social-work/master-of-social-work/Curriculum/socialworkdictionary_updated_2012_oct23.pdf
Jackson, F. (2003). Ethnogenetic layering: A novel approach to determining environmental health risks among children from three U.S. regions. Journal of Children’s Health, 1(3), 369-386. doi.org/10.3109/15417060390254355
Kiang, P. N. (2017). Understanding our perceptions of Asian Americans. Center for Global Education. Retrieved from http://asiasociety.org/education/understanding-our-perceptions-asian-americans
Krieger, N. (2000). Refiguring “race”: Epidemiology, racialized biology, and biological expressions of race relations. International Journal of Health Services, 1(30), 211-216.
Krogstad, J. M., Passel, J. S., and Noe-Bustamante, L. (2022). Key facts about U.S. Latinos for National Hispanic Heritage Month. Retrieved from https://www.pewresearch.org/short-reads/2022/09/23/key-facts-about-u-s-latinos-for-national-hispanic-heritage-month/
Krogstad, J.M., Stepler, R., and Lopez, M.H. (2015, May 12). English proficiency on the rise among Latinos: U.S. born driving language changes. Washington, D.C.: Pew Research Center. Retrieved from http://www.pewhispanic.org/2015/05/12/english-proficiency-on-the-rise-among-latinos/
Lederach, J.P. (1995). Preparing for peace: Conflict transformation across cultures. Syracuse, NY: Syracuse University Press.
Linton, R. (1945). The cultural background of personality. New York: Appleton- Century- Crofts.
Lipka, M. (2017, August 9). Muslims and Islam: Key findings in the U.S. and around the world. Washington, D.C.: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2017/08/09/muslims-and-islam-key-findings-in-the-u-s-and-around-the-world/
Martin, E. P. (1980). The Black extended family. Chicago: University of Chicago Press.
McIntosh, P. (1989). White privilege: Unpacking the invisible knapsack. Retrieved on from https://psychology.umbc.edu/files/2016/10/White-Privilege_McIntosh-1989.pdf
National Association of Social Workers (NASW). (2001). Standards for cultural competence in social work practice. Washington, DC: NASW Press.
National Association of Social Workers (NASW). (2007). Indicators for the achievement of the NASW standards for cultural competence in social work practice. Washington, DC: NASW Press. Retrieved from https://www.socialworkers.org/LinkClick.aspx?fileticket=PonPTDEBrn4%3D
National Association of Social Workers (NASW). (2013, Summer). Families and immigration. A quick resource guide. Washington, DC: NASW Press. Retrieved on from https://www.socialworkers.org/assets/secured/documents/practice/familiesandimmigration.pdf
Park, A. (2016, June). A development agenda for sexual and gender minorities. Los Angeles: The Williams Institute, UCLA School of Law. Retrieved from https://williamsinstitute.law.ucla.edu/wp-content/uploads/Development-Agenda-for-Sexual-and-Gender-Minorities.pdf
Pew Research Survey. (2013, April 4). The rise of Asian Americans. Washington, DC: Pew Research Center. Retrieved from http://www.pewsocialtrends.org/2012/06/19/the-rise-of-asian-americans/
Race, Ethnicity, and Genetics Working Group. (2005). The use of racial, ethnic, and ancestral categories in human genetics research. American Journal of Human Genetics, 77(4), 519-532. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1275602/
Sutton, M. (2004). An introduction to native North America (2nd ed.). New York: Pearson Education, Inc.
United States Census Bureau. (n.d.). U.S. Census Bureau. (n.d.). 2020 Decennial Census. U.S. Department of Commerce. https://data.census.gov/
United States Commission on International Religious Freedom (USCIRF). (2016, April). Burma: USCIRF urges government to end religious freedom abuses [Press release]. Retrieved from http://www.uscirf.gov/news-room/press-releases/burma-uscirf-urges-government-end-religious-freedom-abuses
Useem, J., & Useem, R. (1963). Men in the middle of the third culture: The roles of American and non-western people in cross-cultural administration. Human organizations, 22(3), 169-179. doi.org/10.17730/humo.22.3.5470n44338kk6733
Weaver, H. N. (2008). The elements of cultural competence: Applications with Native American clients. Journal of Ethnic & Cultural Diversity in Social Work, 13(1), 19-35. http://dx.doi.org/10.1300/J051v13n01_02
5
Poverty looks different across the world. Commonly when we think of poverty, we relate it to the images we see on television of malnourished children living in developing countries. However, poverty is all around us. Even though the United States is one of the wealthiest countries in the world, each year millions of Americans live in poverty. The United States Census BureauIn the US in 2021 37.9 million people were living in poverty, 12.8% of the population. (Creamer et al., 2022). A wide array of Americans from all races, ethnicities, ages, backgrounds, and geographic locations makes up the 43.1 million people currently living in poverty. Some groups are more vulnerable to poverty. The most vulnerable groups make up most of the impoverished population (Rodgers, 2015). The groups that are more susceptible to suffer poverty include single parent families especially those headed by women), minorities, unemployed or under- employed adults, individuals with mental illness or disabilities, and the elderly (Rodgers, 2015). An example of what living in poverty looks like in America is a single parent who works full time, but still cannot afford to pay for food, rent, childcare, medical bills, and the costs of transportation to work (Results, 2017). Poverty is said to be America’s most serious and costly social problem (Rodgers, 2015).
Although poverty is one of the most familiar and enduring conditions known to humanity, it is a highly complicated concept to understand fully. To date there is no one standard definition of poverty, but numerous definitions and descriptions exist. All current definitions and descriptions agree that poverty is a complex societal problem. It is important that all members of our society work together to provide opportunities for all members to reach their full potential. It helps all of us to help one another.
When discussing poverty, the terms absolute poverty and relative poverty are often used (Iceland, 2013). Absolute and relative are the two most common forms of poverty delineated in our society and around the world (Pierson & Thomas, 2010).
ABSOLUTE POVERTY refers to the amount of money necessary to meet basic needs such as food, clothing, and shelter. The concept of absolute poverty is not concerned with the broader quality of life issues or with the overall level of inequality in society but is based strictly on whether or not basic needs are being met (UNESCO, 2017). Examples of absolute poverty would include not knowing when or where your next meal will come from, not having access to clean drinking water, and not having an adequate place to sleep each night.
RELATIVE POVERTY refers to the lack of resources to obtain the types of diet, participate in the activities, and have the living conditions and amenities that are customary to maintain the average standard of living in society (Pierson, & Thomas, 2010; Poverty eradication, 2012). Relative poverty defines poverty in relation to the economic status of other members of society, therefore determining if people are poor by gauging if they fall below normal standards of living in a given society (UNESCO, 2017). Examples of relative poverty would include not being able to have your children participate in after school activities, not being able to afford to dine out, or not being able to take vacations.
In the United States, there are two official poverty measures. Poverty thresholds are the primary version of the federal poverty measure and the second measure being poverty guidelines.
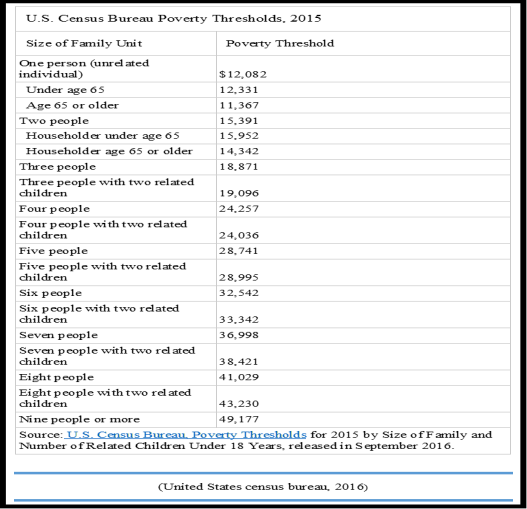
POVERTY THRESHOLDS were developed in the mid-1960s by determining the cost of a minimum food diet and then multiplied the cost by three to account for other family expenses (United States Census Bureau, 2016). The U.S Census Bureau updates the threshold annually to account for inflation using the Consumer Price Index (Institute for Research on Poverty, 2016). Currently, the U.S. Census Bureau determines poverty status by comparing pre-tax cash income against the threshold that has been set for that year (see Figure 1) (Institute for Research on Poverty, 2016). If the family’s total income is less than the family’s threshold, then that family and every individual in it is considered to be living in poverty (United States Census Bureau, 2016). Based on the poverty threshold data it was concluded there were 43.1 million people in the United States living in poverty in 2015 (Institute for Research on Poverty, 2016; Proctor, Semega, & Kollar, 2016).
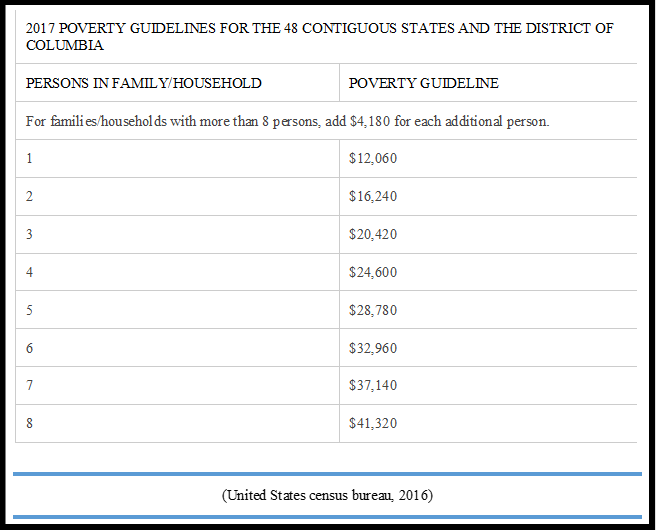
POVERTY GUIDELINES are the other official federal poverty measure used in the United States. Updated poverty guidelines are issued every year by the U.S. Department of Health and Human Services (DHHS) (Institute for Research on Poverty, 2016). Udated guidelines take economic changes into account. The poverty guidelines are a simplification of poverty thresholds utilized to determine an individual’s eligibility for select federal programs (DHHS, 2017).
Examples of federal programs that use poverty guidelines to determine eligibility include the following:
(Institute for Research on Poverty, 2016)
Even though the current official poverty measures have been used consistently since the 1960s, there are widespread concerns that the federal poverty measure is flawed. There is an overarching agreement that the Census Bureau does not identify all individuals living in poverty. The Census Bureau is unable to obtain exact numbers because many low-income individuals live with others or are frequently moving and are in many cases homeless. Furthermore, those residing in psychiatric hospitals, college dorms, nursing homes, serving in the military, and/or in jails or prisons are not counted. It is estimated that several million individuals who would fall below the poverty threshold and poverty guidelines are not counted each year (Rodgers, 2015).
Each year hundreds of billions of public and private dollars are spent on efforts to prevent poverty and assist those living in poverty (Rodgers, 2015). According to the United States Census Bureau in 2020, there were approximately 69.8 million people in the United States receiving some sort of assistance through government-funded welfare programs (Social Security Administration, 2021).
The welfare system in the United States consists of government programs which provide financial assistance to individuals and families who cannot support themselves. Welfare programs are funded by taxpayers and allow people to cope with financial stress during challenging periods of their lives. The goals of welfare include the attainment of:
To receive assistance from government funded programs individuals must meet a certain criterion to be eligible. Each program has its own distinct criteria. If individuals do not qualify, they do not receive assistance and would need to seek assistance from somewhere else. To apply to these programs individuals must go through state Departments of Health and Human Services (DHHS).
The United States laid its foundation for a national welfare system in response to the Great Depression that started in 1929 and went through most of the 1930s. The Social Security Act of 1935 was the first of many government policies and welfare programs created to combat poverty and economic hardships (Rodgers, 2015). Since the establishment of Social Security Act of 1935, the federal government has continued to develop numerous welfare programs to attempts to eradicate poverty and the economic hardships faced by millions of Americans. Key programs to combat poverty include but are not limited to the following:
All information is from the Center for Poverty Research
In the United States individuals living in poverty are not only faced with their day-to-day hardships but also with the harsh stigmas that society has surrounding poverty. When evaluating stigmas surrounding poverty, they typically fall into three categories: institutional, social, and personal stigmas (Bell, 2012; Inglis, 2016):
Furthermore, society holds many stereotypes about individuals living in poverty. A stereotype can be defined as an often unfair and untrue belief that many people have about all people with a specific characteristic (Stereotype, 2017). The stereotypes that society has labeled individuals living in poverty are usually false. Some of the most common stereotypes and misconceptions of individuals living in poverty include:
Stigmatizing and stereotyping individuals living in poverty only further creates a divide between low-income people who are living in poverty and those who are not (Inglis, 2016). Society’s harsh views on poverty cause impoverished individuals to further feel socially excluded and ashamed of the situation they are in. Research has shown negative effects on an individual’s self-esteem, self-concept, and mental and physical health due to being stigmatized and stereotyped so severely by society (Inglis, 2016).
There are many theories that attempt to explain poverty and why it exists. The following are some of the most commonly used theories to explain the existence of poverty.
Social workers abide by the National Association of Social Work (NASW) Code of Ethics. One of the six values in the NASW code of ethics is social justice. The definition of the ethical principle from the NASW states, “Social workers’ social change efforts are focused primarily on issues of poverty, unemployment, discrimination, and other forms of social injustice,” (NASW, 2008). With the NASW Code of Ethics acting as the profession’s guiding light, it is highly important for social workers to have knowledge and understanding of poverty and its severity within our society and around the world.
While the US is one of the wealthiest nations in the world, tens of millions of people live in poverty. Despite government programs and interventions, poverty persists and often falls on the most vulnerable populations. Therefore, Social Work is committed to serving those experiencing poverty and advocating for social change to provide more resources and opportunities. If Social Work is your intended career path, it is important to recognize that you will serve individuals and families who fall below the poverty line and face financial hardships. Therefore, as future social workers it is important that you have an adequate understanding of what poverty is and the effects it has on individuals and society as a whole.
Ban der Berg, S. (2008). Poverty and education. Retrieved from https://unesdoc.unesco.org/ark:/48223/pf0000181754
Bell, Kate. (n.d.). Poverty, social security, and stigma. Poverty, 144, 10-13. Retrieved from http://www.cpag.org.uk/sites/default/files/CPAG-Povertyarticle-stigma-0213.pdf
Center for Poverty Research, University of California, Davis. (2017). What are the major federal safety net programs in the U.S.? Retrieved from https://poverty.ucdavis.edu/article/war-poverty-and-todays-safety-net-0
Creamer, J., Shrider, E. A., Burns, K., & Chen, F. (2022) Poverty in the United States: 2021. Retrieved from https://www.census.gov/library/publications/2022/demo/p60-277.html
Giffords, E. D., & Garber, K. R. (2014). New Perspectives on poverty: Policies programs and practice. Chicago: Lyceum Books.
Gorski, P. C. (2013). Reaching and teaching students in poverty: Strategies for erasing the opportunity gap. New York: Teachers College Press.
Harack, B. (2010, October 5). How do we define poverty? Vision of earth. Retrieved from https://www.visionofearth.org/news/how-do-we-define-poverty/
Health Resource & Service Administration. (2017). Health center program terms and definitions. Retrieved from https://www.hrsa.gov/grants/apply/assistance/Buckets/definitions.pdf
Henry, M., Watt, R., Rosenthal, L., & Shivji, A. (2016, November). The 2016 annual homeless assessment report (AHAR) to Congress. Washington, DC: U.S Department of Housing and Urban Development. Retrieved from https://www.huduser.gov/portal/sites/default/files/pdf/2016-AHAR-Part-2.pdf
Iceland, J. (2013). Poverty in America. Berkeley: University of California Press.
Inglis, G. (2016, October 19). The stigma of poverty. The Poverty Alliance. Retrieved from https://povertyalliance.wordpress.com/2016/10/19/the-stigma-of-poverty/
Institute for Research on Poverty, University of Wisconsin. (2017). What are poverty thresholds and poverty guidelines? Retrieved from https://www.irp.wisc.edu/resources/what-are-poverty-thresholds-and-poverty-guidelines/
International Federation of Social Workers. (2012, February 23). Poverty eradication and the role for social workers. Retrieved from http://ifsw.org/policies/poverty-eradication-and-the-role-for-social-workers/
Kirst-Ashman, K. (2012). Introduction to social work and social welfare [4th ed.]. Pacific Grove, CA: Brooks Cole.
National Alliance to End Homelessness. (2010, January 17). Rural homelessness. Retrieved from http://endhomelessness.org/resource/rural-homelessness/
National Alliance to End Homelessness. (2016). Housing. Retrieved from http://endhomelessness.org/homelessness-in-america/what-causes-homelessness/housing/
National Association of Social Workers (NASW). (2021). Code of Ethics of the National Association of Social Workers. Retrieved from http://www.socialworkers.org/pubs/code/code.Asp
National Health Care for Homeless Council. (2022). What is the official definition of homelessness? Retrieved from https://nhchc.org/understanding-homelessness/faq/
Pierson, J., & Thomas, M. (2010). Dictionary of social work: The definitive A to Z of social work and social care. New York: Open University Press.
Proctor, B. D., Semega, J. L., & Kollar, M. A. (2016, September). Income and poverty in the United States: 2015. (States Census Bureau, Report #P60-256). Retrieved from https://www.census.gov/library/publications/2016/demo/p60-256.html
Results: The Power to End Poverty. (2017). Poverty in the United States. Retrieved from https://results.org/#
Ritter, J. A. & Vakalahi, H.F.O. (2014). 101 careers in social work [2nd ed.]. New York, NY: Springer Publishing Company.
Rodgers, H. R. (2015). American poverty in a new era of reform [2nd ed.]. Armonk, NY: Taylor and Francis. Social problems: Continuity and change. (2010). Minneapolis: University of Minnesota Libraries. https://doi.org/10.24926/8668.2301
Social Security Administration (2021). Fast Facts & Figures About Social Security, 2021. Office of retirement and disability policy. Retrieved 4/25/23 from https://www.ssa.gov/policy/docs/chartbooks/fast_facts/2021/fast_facts21.html
Stereotype. (2017). Merriam-Webster’s learner’s dictionary. Retrieved from http://www.learnersdictionary.com/definition/stereotype
Sue, D. W., Rasheed, M. N., & Rasheed, J. M. (2012). Multicultural social work practice: A competency- based approach to diversity and social justice [2nd ed.]. Hoboken, NJ: Wiley.
Theory. (2017). Merriam-Webster’s learners dictionary. Retrieved from http://www.learnersdictionary.com/definition/theory
Tropman, J.E. (2021). Micro, mezzo (meso), and macro: A guide to the three levels of social work. Retrieved from https://mastersinsocialworkonline.org/resources/levels-of-social-work/
United States Census Bureau. (2016, August). The history of the official poverty measure. Retrieved from https://www.census.gov/topics/income-poverty/poverty/about/history-of-the-poverty-measure.html
United States Department of Health & Human Services (DHHS). (2017). U.S. federal poverty guidelines used to determine financial eligibility for certain federal programs. Retrieved from https://aspe.hhs.gov/poverty-guidelines
The World Bank. (2015, September 30). FAQs: Global poverty line update. Retrieved from http://www.worldbank.org/en/topic/poverty/brief/global-poverty-line-faq
6
Learning Objectives
In this chapter the student will be reviewing:
Social Work practice begins with the purpose of the social worker. Understanding of the social work profession starts with an intense appreciation of the person in which the social worker serves (Sheafor & Horejsi, 2008). The social worker understands that humans are social beings, these social creatures’ growth and development need the guidance of nurturing and protection provided by others around them. It is this inter-connectedness and interdependence of people in the social environment that is the foundation of practice in social work as a profession. The environment a person lives in has a lot to do with how a social worker may apply knowledge and guidance. There are two distinct types of social work practice that are used according to the type of setting.
Direct practice is when the social worker works directly with an individual, family, or group of people. The first direct meeting can occur in a variety of ways such as a crisis, voluntary, or involuntary. The first meeting is a critical point in establishing a good helping relationship. A social worker should prepare for any type of first contact, so that they may set up the best relationship possible with the client (Sheafor & Horejsi, 2008).
At the BSW level, direct practice is primarily done as a case worker. The case worker may meet with the individual daily, weekly, or monthly depending on the type of work. For example, in short term crisis work, the person may have daily meetings. For adults with intellectual disabilities, a monthly check-in may be more appropriate and required by the supervising agency. Direct practice is typically done as a worker at an agency, non- profit, or government setting. A direct case worker may be involved in many different areas of practice, including but not limited to working in adoption, Child Protective Services, in a group home for individuals with brain injuries, a shelter for abuse survivors, or with Community Mental Health. The caseworker may be involved in finding resources or providing support for the client. Meetings may take place at an agency or in the client’s home.
At the MSW level, direct practice is usually done in the role of the therapist or counselor. Therapists see their clients on a weekly basis, although this period may vary. Therapists often work at the same agencies as BSW level caseworkers, but in a different role. While the BSW worker is involved with taking care of the many logistical issues a client may have (housing, food, etc.), the MSW worker is usually assisting the client with skill building, learning coping strategies, and focusing on their overall mental health treatment. Sessions may take place at an agency or in the client’s home.
Indirect practice is generally when the social worker is involved in activities that consist of facilitating change through programs and policies. This type of practice is more of behind the scenes and is aimed to help prevent problems from developing. Also, the social worker may participate in this type of practice by advocating through agency administrators, legislators, or other powerful people to effect a change (Sheafor & Horejsi, 2008). You may also hear the term Macro system practice, which means systems larger than a small group or single person (Zastrow & Kirst-Ashman, 2010). Micro systems are continuously affected by the Macro systems. The two major Macro systems that impact individuals the most are communities and organizations.
According to an article written by Johnson (1999), Indirect social practice has often referred to environmental intervention in the client’s networks or social aspect. The belief was to help alleviate challenges in the client’s surroundings. There are two elements associated with indirect practice. The first one is called concrete assistance; this is resources available to the client to help with basic needs. For example, food assistance programs are the most common resource needed for clients. The second element to indirect social work practice is sociopsychological intervention. Which is the adjustment of attitude or behavior of significant people within the client’s social environment (Johnson, 1999).
Such limited resources in consideration include available locations, trained and licensed individuals, and monetary funds. Thus, as Lohmann (2011) describes, social workers must play multiple roles, from community organizers to caseworkers. As such, these roles are valued for their creativity in how treatment occurs, and how flexible the social worker is with switching between the individual and the community. Limited resources also mean that rural social workers often practice in isolation, without direct supervision and with difficulty accessing continuing educational materials. As such, it is important that these workers seek additional opportunities to expand their professional development and continue advocating for best practices.
In contrast to rural communities, urban communities are those settings involving metropolitan areas with an increase in population density, a decrease in general size, and an increase in access to social services for its population. The rise of industrialization has led to a migration from rural communities to urban ones, resulting in a population shift between the two areas where urban areas hold much of the population. This, in term, leads to an increase in problems, such as differences in socioeconomic status, an increase in migrant and immigrant populations, higher crime rates, and differences in health outcomes of residents.
Unlike rural environments, urban environments allow for a range of continual educational options, including seminars at meeting halls or college campuses, specialized opportunities for trainings in issues such as a trauma, and the ability for social workers to gather in conferences. This, in turn, allows social workers to have outside supervision, as well as an increase in communication across the profession.
BSW- Bachelor of Social Work: this is considered an Undergraduate degree and is an employable degree once you gain your Limited License. If you choose not to move on to a Graduate degree you will need to take the state licensing exam to practice a career in what you have learned. Your employment at the BSW level will be related to casework. Many individuals work with just their BSW for their entire lives. If you enjoy casework, it is not necessary to obtain your MSW degree. There are many positions available for BSW level workers.
MSW- Master of Social Work: this is considered a graduate degree and is employable with a Limited License. If you choose to stay with your MSW you can take the licensing exam in the state, you are choosing to practice in and follow your state’s guidelines for licensure and procure a clinical or macro licensure.
Now that we have covered distinctions of the BSW and MSW degrees, and the urban and rural work settings, let us move on to a vital part of working in the field: state licensure. It is important to keep in mind that all states and countries are different with regulations regarding licensure for practice. The same goes for BSW and MSW criteria for licensure. What we are offering in this text are the requirements for the LBSW, LMSW, and LCSW in the State of Texas.
Overall, here is what is required for Texas licensure at the present time. This information is shared with the caveat that changes are made periodically by the Texas State Board of Social Work Examiners. To be eligible to become a social worker in Texas, you must have graduated from a Council on Social Work Education-accredited program (CSWE) with a bachelor’s or master’s degree in Social Work and have passed the applicable Association of Social Worker Board (ASWB) licensing exam.
A presentation offered by Professor Karen Magruder on the Texas Licensure process:
2020 Presentation on Texas Licensure by Professor Karen Magruder
All applicants must:
Applicants licensed as a social worker in another state must also submit official verification of license from every state in which a social worker license is/was held. Applicants who have not yet taken the licensing exam begin the process by applying for the exam with ASWB. Information on that process is available on our ASWB Licensure Examinations webpage.
The requirements for obtaining a license as a Licensed Baccalaureate Social Worker are set forth in 22 TAC 781.401. These requirements include:
The requirements for obtaining licensure as a Licensed Master Social Worker are set forth in 22 TAC 781.401. These requirements include:
The requirements for obtaining licensure as a Licensed Clinical Social Worker are set forth in 22 TAC 781.401. These requirements include:
Anderson, R. E., Carter, I., & Lowe, G. R. (2008). Human behavior in the social environment a social system approach. Piscataway, NJ: Transaction.
Ashford, J. B., Lecroy, C. W., & Lortie, K. L. (2006). Human behavior in the social environment a multidimensional perspective. Belmont, CA: Thomson.
Community. (n.d.). Merriam-Webster. Retrieved from https://www.merriam-webster.com/dictionary/community
Donaldson, L. P., Hill, K., Ferguson, S., Fogel, S., & Erickson, C. (2014). Contemporary social work licensure: Implications for macro social work practice and education. Social Work, 59(1), 52-61.
Dulmus, C. N, & Sowers, K. M. (Eds.) (2012). The profession of social work: Guided by history, led by evidence. Hoboken, NJ: Wiley & Sons.
Humble, M., Lewis, M., Scott, D., & Herzog, J. (2013). Challenges in rural social work practice: When support groups contain your neighbors, church members, and the PTA. Social Work with Groups, 36(2-3), 249-258.
Johnson, Y. (1999). Indirect work: Social work’s uncelebrated strength. Social Work, 44(4), 323-334.
Lee, W. (2016). Social work-business sector collaboration in pursuit of economic justice. Social Work,61(3), 209-16.
Lightburn, A., & Sessions, P. (2005). Handbook of community-based clinical practice. Cary, NC: Oxford University Press.
Lohmann, N., & Lohmann, R. A. (Eds.) (2012). Rural social work practice. New York: Columbia University Press.
Pugh, R. (2007). Dual relationships: Personal and professional boundaries in rural social work. British Journal of Social Work, 37, 1405-1423.
Lishman, J. (Ed.) (2011). Social work education and training. London: Jessica Kingsley Publishers.
Sheafor, B. W., & Horejsi, C.R. (8). (2008). Techniques and guidelines for social work practice. Boston, MA: Pearson Education.
Schilling, R., Morrish, J., & Liu, G. (2008). Demographic trends in social work over a quarter-century in an increasingly female profession. Social Work,53(2), 103-14.
Texas Behavioral Health Executive Council: https://www.bhec.texas.gov/index.html
Waltman, G. (2011). Reflections on rural social work. Families in Society: The Journal of Contemporary Social Services, 92(2), 236-239.
Zastrow, C. H., & Kirst-Ashman, K. K. (2010). Understanding human behavior and the social environment. Belmont, CA: Brooks/Cole.
7
Learning Objectives
In this chapter, the student will be reviewing the following:
When looking at generalist practice primary theories, the first question that may come to mind is what is generalist practice? Generalist practice introduces students to the basic concepts in social work which includes promoting human well-being and applying preventative and intervention methods to social problems at individual (micro), group (mezzo), and community (macro) levels while following ethical principles and critical thinking (Inderbitzen, 2014).
Now that you have some insight into what generalist practice is, we should discuss what a social work generalist does. A social work generalist uses a wide range of prevention and intervention methods when working with families, groups, individuals, and communities to promote human and social well-being (Johnson & Yanca, 2010).
Being a social work generalist practitioner prepares you to enter any profession within the social work field, depending on your population of interest (Inderbitzen, 2014). Some professions within the social work field include but are not limited to Medical social worker, school social worker, community outreach, human services, etc.
MICRO: Micro level social work is the most widespread practice scenario and happens directly with an individual client or family; in most cases this is case management and therapy service. Micro social work involves meeting with individuals, families, or small groups to help identify, and manage emotional, social, financial, or mental challenges, such as helping individuals to find appropriate housing, health care, and social services.
MEZZO: The major difference between micro and mezzo level social work is that instead of engaging in individual counseling and support, mezzo social workers administer help to groups of people. There are many diverse types of groups that involve social workers: task, therapy, education, self-help, support, and psychoeducation. The following is a brief description of these types of groups:
MACRO: Macro level social work is very distinct from micro and mezzo level. The focus of macro level social work is to help vulnerable populations indirectly and on a larger scale. The responsibilities for social workers on a macro level typically are finding the root cause or the why and effects of citywide, state, and/or national social problems.
Social workers that work on the macro level are often employed at non-profit organizations, public defense law firms (working pro-bono cases), government departments, and human rights organizations.
In individual therapy, also known as individual psychotherapy or individual counseling, the client and clinician meet one-on-one (usually from 45 minutes to 1 hour). These meetings typically occur weekly or every other week, and sessions are conducted in a confidential and caring environment (Figure). The clinician will work with clients to help them explore their feelings, work through life challenges, identify aspects of themselves and their lives that they wish to change, and set goals to help them work towards these changes. A client might see a clinician for only a few sessions, or the client may attend individual therapy sessions for a year or longer. The amount of time spent in therapy depends on the needs of the client as well as the client’s personal goals.
Family therapy is a special form of group therapy, consisting of one or more families. Although there are many theoretical orientations in family therapy, one of the most predominant is the systems approach. The family is viewed as an organized system, and everyone within the family is a contributing member who creates and maintains processes within the system that shape behavior (Minuchin, 1985). Each member of the family influences and is influenced by the others. The goal of this approach is to enhance the growth of each family member as well as that of the family.
Questions and compliments are the primary tools of the solution-focused approach. SF therapists and counselors deliberately refrain from making interpretations.[3] and rarely confront their clients. Instead, they[3] focus on identifying the client’s goals, generating a detailed description of what life will be like when the goal is accomplished, and the problem is either gone or coped with satisfactorily. To develop effective solutions, they search diligently through the client’s life experiences for “exceptions”, e.g., times when some aspect of the client’s goal was already happening utilizing these to co-construct uniquely appropriate and effective solutions.[10]
This is not so much a specific change model as it is lens for the change process in general. Such a perspective suggests that our change models have exclusively been grounded in a European, monocultural perspective. As such there has been a disregard for more multicultural worldviews as related to change orientations. However, as has been noted about the NASW (National Association of Social Workers) Code of Ethics, it is the responsibility of the culturally competent social worker to offer a “set of knowledge, behaviors, attitudes, skills, and policies that enables a practitioner to work effectively in a multicultural situation.”
What might be some interventions that reflect such multicultural sensitivities? The social worker might include the following in their multicultural practice:
The narrative therapist focuses upon assisting people to create stories about themselves, about their identities, that are helpful to them. This work of “re- authoring identity” claims to help people identify their own values and identify the skills and knowledge they must live these values. Through the process of identifying the history of values in people’s lives, the therapist can co-author a new story about the person.[6]
Play therapy is often used with children since they are not likely to sit on a couch and recall their dreams or engage in traditional talk therapy. This technique uses a therapeutic process of play to “help clients prevent or resolve psychosocial difficulties and achieve optimal growth” (O’Connor, 2000, p. 7). The idea is that children play out their hopes, fantasies, and traumas while using dolls, stuffed animals, and sandbox figurines (Figure). Play therapy can also be used to help a therapist make a diagnosis. The therapist observes how the child interacts with toys (e.g., dolls, animals, and home settings) to understand the roots of the child’s disturbed behavior.
Cognitive therapy is a form of psychotherapy that focuses on how a person’s thoughts lead to feelings of distress. The idea behind cognitive therapy is that how you think determines how you feel and act. Cognitive therapists help their clients change dysfunctional thoughts to relieve distress. They help a client see how they misinterpret a situation (cognitive distortion). For example, a client may overgeneralize. Because Ray failed one test in his Psychology 101 course, he feels he is stupid and worthless. These thoughts then cause his mood to worsen. Therapists also help clients recognize when they blow things out of proportion. Because Ray failed his Psychology 101 test, he has concluded that he is going to fail the entire course and flunk out of college altogether. These errors in thinking have contributed to Ray’s feelings of distress. His therapist will help him challenge these irrational beliefs, focus on their illogical basis, and correct them with more logical and rational thoughts and beliefs.
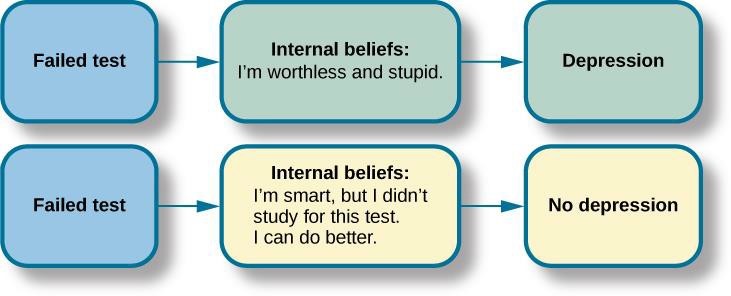
Cognitive-behavioral therapy aims to change cognitive distortions and self- defeating behaviors using techniques like the ABC model. With this model, there is an Action (sometimes called an activating event), the Belief about the event, and the Consequences of this belief. Let us say, Jon and Joe both go to a party. Jon and Joe each have met a young woman at the party: Jon is talking with Megan most of the party, and Joe is talking with Amanda. At the end of the party, Jon asks Megan for her phone number and Joe asks Amanda. Megan tells Jon she would rather not give him her number, and Amanda tells Joe the same thing. Both Jon and Joe are surprised, as they thought things were going well. What can Jon and Joe tell themselves about why the women were not interested? Let us say Jon tells himself he is a loser, or is ugly, or “has no game.” Jon then gets depressed and decides not to go to another party, which starts a cycle that keeps him depressed. Joe tells himself that he had bad breath, goes out and buys a new toothbrush, goes to another party, and meets someone new.
The following are examples of irrational beliefs:
What do you think?
Review the list of more common irrational beliefs and pick out one or two could cause you a negative or distressed reaction to an activating event (as noted above).
The Systems Theory is valuable to the social work profession because it assists social workers with identifying, defining, and addressing problems within social systems. As social workers, we utilize Systems Theory to help us understand the relationships between individuals, families, and organizations within our society. Systems theory allows social workers to identify how a system functions and how the negative impacts of a system can affect a person, family, organization, and society, by working together to cause a positive impact within that system (Flamand, 2017).
Related to the Systems’ theory is the ecological systems theory. The main concept behind ecological approach is “person in environment” (P.I.E). The ecological approach implies that every person lives in an environment that can affect their outcome or circumstance. As social workers, our job is to improve a person’s environment by helping them identify what is negatively impacting their environment.
An eco-map is a diagram that shows the social and personal relationships of an individual with his or her environment. Eco-maps were developed in 1975 by Dr. Ann Hartman, a social worker who is also credited for developing the genogram (Genachte, 2009). Eco-maps will vary in what they look like as each map will cater to the specific client/family, and will highlight the stressors (negatives), positives, and relationships.
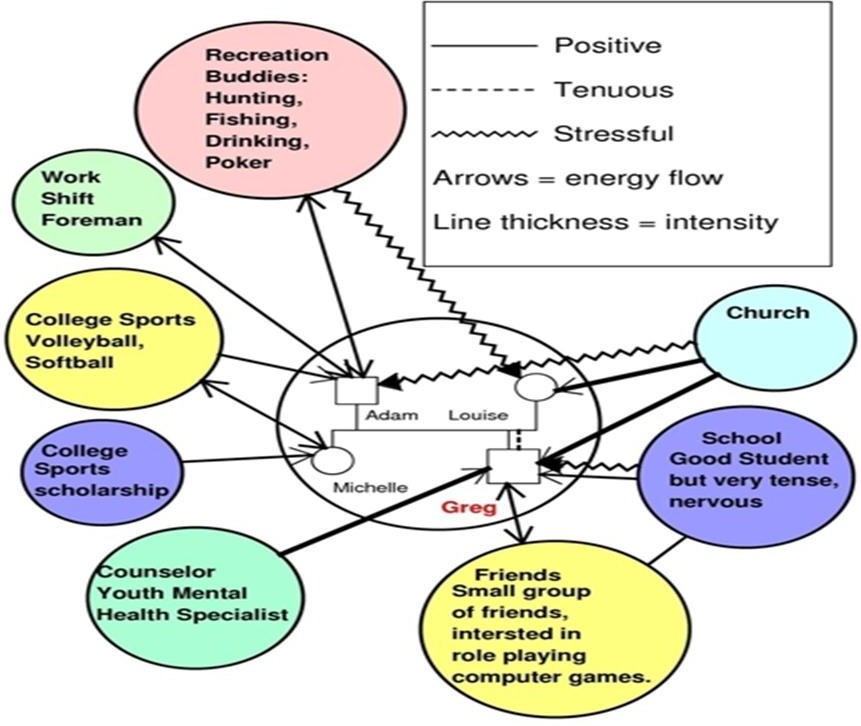
A genogram mimics a family tree. Normally when you look at a family tree you often find branches and each branch represents a family. A genogram digs deeper and identifies relationships, deaths, marriages, births, divorce, and adoptions just to name a few. When collecting information to complete a genogram it is useful to understand a family’s dynamics (Johnson & Yanca, 2010.)
Here is an example of a genogram; this genogram along with other samples and variations can be found on www.sampletemplates.com. Genograms can help clients identify their roots and culture. While completing genograms also be aware that while unraveling a client’s history, past trauma or closed wounds can be reopened. As a social worker you need to be prepared to discuss and address these issues to help your client address their past trauma.
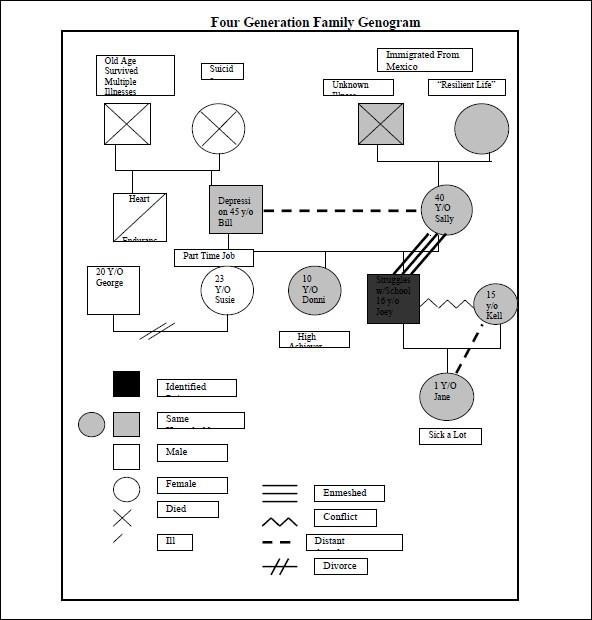
What do you think?
In class or as homework complete and eco map and genogram of your own family. See how far you can go through family tree and connect your family, relationships, marriages, etc.
The development of the Strengths Approach began and has been led by Dennis Saleeby and staff at the University of Kansas. The Strengths Approach is based off two especially important principles:
In the Strengths Approach, it is the social worker’s job to help the client identify their strengths. Often clients with whom we work are only able to identify the negative impacts of their lives and have a tough time identifying the positive aspects of their lives and situations. When using the Strengths Approach not only is the social worker helping the client to identify their personal strengths, but the worker is also helping the client identify local resources to help the client needs.
The planned change process was introduced to the social work profession in 1957 by Helen Harris Perlman. The Planned Change Model is the development and implementation of a plan or strategy to improve or alter a pattern of behaviors, a condition, or circumstance to improve a client’s well-being or situation (Kirst- Ashman, 2012).
The Planned Change Model consists of a seven-step process which includes:
ENGAGEMENT: The Engagement phase is the first interaction between the social worker and their client. The engagement stage does not have a predetermined period; it can last for a couple of minutes to a few hours depending on the client and the circumstances. It is especially important during the engagement phase that the social worker displays active listening skills, eye contact, empathy, and empathetic responses, can reflect to the client what has been said, and uses questioning skills (motivational interviewing).
ASSESSMENT: The Assessment phase is the process occurring between social worker and client in which information is gathered, analyzed, and synthesized to provide a concise picture of the client and their needs and strengths. The assessment phase is especially important as it is the foundation of the planning and action phases that follow.
During the assessment stages, there are five key points:
PLANNING: The Planning phase is when the client and social worker develop a plan with goals and objectives as to what needs to be done to address the problem. A plan is developed to help the client meet their needs or address the problem (Johnson, & Yanca, 2010). The planning phase is a joint process where the worker and the client identify the strengths and resources gathered from the assessment phase. Once the strengths and resources are identified, the social worker and the client produce a plan by outlining goals, objectives, and tasks to help meet the client’s goal to address the need or problem. During the planning phase, keep in mind that the goals should be what the client is comfortable with and finds feasible to obtain. The social worker’s most important job during this phase is to help the client identify strengths and resources, not to produce the client’s goals for them.
IMPLEMENTATION: The Implementation/Action phase is when the client and social worker execute a plan to address the areas of concern by completing the objectives to meet the client’s goals. The action phase is also considered a joint phase as the social worker and the client act! The worker and the client begin to work on the task that were identified in the planning phase (Johnson & Yanca, 2010). The worker and the client are responsible for taking on various parts of the identified task; for example, the social worker may find a local food pantry or help with food assistance program if the client needs food. The client may work on making a grocery list of foods that will make bigger portions for leftovers to make food last longer for the family. However, the worker and the client are jointly working together to obtain the goal of providing food for the client and their family.
TERMINATION: The Evaluation Phase/Termination phase is constant. The worker should always evaluate how the client is doing throughout the process of the working relationship (Johnson & Yanca, 2010). When the plan has been completed or the goals have been met, the client and social worker review the goals and objective and evaluate the change and/or the success. If change or progress has not been made the client and social worker review the goals and objectives and make changes or modifications to meet the goal. Once the goals have been met, termination of services follows if there is no further need for services or other concerns to address. Sometimes termination happens before goal completion, due to hospitalizations, relocation, losing contact with a client, financial hardships, or the inability to engage the client.
The Follow Up phase is when the social worker reaches out to the client to make sure they are still following their goals, using their skills, and making sure the client is doing well. The follow up may not always be possible due to different situations such as death, relocation, and change in contact information, to name a few.
The diagram below shows the process of the Planned Change Model when working with clients.
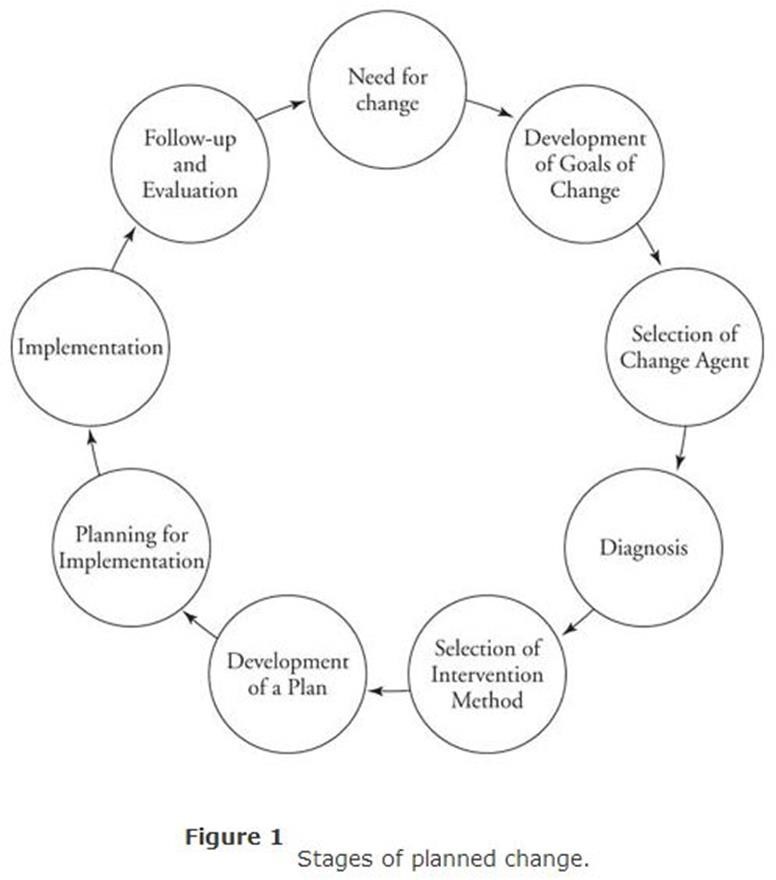
Activity: Partner up with a classmate. Role plays one person being the social worker and the other being the client. Produce a problem or concern and try to go through the planned change process. I do not expect you to get through the entire process, but at least try to get through the first three stages. Remember to be creative and have fun while doing so!!
Allen-Meares, P., & Lane, B. (1987). Grounding social work practice in theory: Ecosystems. Social Casework, 68, 515-521.
Bonecutter, & Gleeson. (n.d.). Genograms and ecomaps: Tools for developing a broad view of family. Retrieved from https://tnchildren.org/wp-content/uploads/2014/11/Genograms-and-Ecomaps.pdf
Dziegielewski, S. (2013). The changing face of health care social work (3rd ed.). New York: Springer.
Elements Behavioral Health. (2012, August 10). What are evidence-based practices? Retrieved from https://www.elementsbehavioralhealth.com/addiction-recovery/evidence-based-practices/
Flamand, L. (2017). Systems theory of social work. People of everyday life. Retrieved from http://peopleof.oureverydaylife.com/systems-theory-social-work-6260.html
Inderbitzen, S. (2014, February 3). What does it mean to be a social work generalist? Social work degree guide. Retrieved from http://www.socialworkdegreeguide.com/what-does-it-mean-to-be-a-social-work-generalist/
Johnson, L. C., & Yanca, S. J. (2010). Social work practice: A generalist approach (10th ed.). Boston, MA: Allyn & Bacon.
Kirst-Ashman, K. K., & Hull, G. H., Jr. (2015). Generalist practice with organizations and communities (6th ed.). Pacific Grove, CA: Brooks/Cole.
Lewin, R. G. (2009). Helen Harris Perlman. In Jewish women: A comprehensive historical encyclopedia. Retrieved from https://jwa.org/encyclopedia/article/perlman-helen-harris
Pardeck, J. T. (1988). An ecological approach for social work practice. The Journal of Sociology & Social Welfare, 15(2), 134-144. Retrieved from http://scholarworks.wmich.edu/jssw/vol15/iss2/11
Steyaert, J. (2013, April). Ann Hartman. In History of social work. Retrieved from www.historyofsocialwork.org
8
Learning Objectives
In this chapter the student will be reviewing:
In this chapter, you will learn about child welfare and foster care, 2 prominent fields of practice for social workers. We will be considering the ever-changing variations of family structure, and the importance for social workers to know their own pre- conceived notions of what it means to be “family.” There will be a brief overview of family systems’ thinking and key concepts. A look at child protective services, and, finally, a consideration of the impact of trauma on a child.
The family systems’ perspective fits well into the core social work perspective, person-in-environment. This perspective is believed to be one of the unique, defining features for social work. As is evident in its name, this concept emphasizes the importance of viewing the individual within the context of their environment. Related to person-in-environment, the family systems’ perspective posits that our view of selves and the world is constantly being informed and influenced by our family, our culture, and other external factors, such as religion, gender, sexual orientation, race, and ethnicity, to name some important ones.
Family systems’ makes several assumptions:
Let us consider some important family systems’ concepts:
The family structure is ever changing and can have various effects on the family as they move forward. A traditional family, also known as nuclear family, is defined by Es (2007) as a married couple and their biological children. This is one of the more reinforced family structures in the dominant society. It should be noted that a child starts out with their traditional family, and as they grow, becomes more involved in outside activities, or even moves out to live with others. Thus, the family grows to beyond relatives and includes friends. Another thing to keep in mind is the idea that a child may start out in one type of family structure and then the structure or dynamic of that family may change due to divorce, death, parents marrying again, or even just an addition to the family through adoption, foster care and more.
Such a discussion on family structure begs the question: how do you define family? When you are asked “who is in your family,” how do you respond? Does your definition of family focus on biological ties or the shared history? Would you consider close friends to be “family?”
In the field of social work, it is incredibly important to remember that we are to validate the families we work with and not judge them. We must acknowledge the family’s culture by respecting their belief systems and values. For example, if a family comes to you and you notice that the female is looking down and not making eye contact, consider the fact that in their culture that may be how the female shows respect to her husband, and other authoritative figures. Thus, interacting with the family in the way they feel comfortable (i.e., talking to the husband first etc.) will help one build a solid rapport (close relationship) with the family group.
Enrique et al. (2007), provides the following ideas for working with families:
Working with Families
Child welfare is necessary in our society to help maintain child safety and keep families working cohesively. The Child Welfare Information Gateway (CWIG) (http://www.childwelfare.gov) Defines child welfare as a field of services that aims to protect children and ensure families have the tools to care for their children successfully. Many people see this happen through an agency like the Department of Health and Human Services (DHHS) which is present in every state. To ensure the safety of children, DHHS is responsible for performing various tasks. These tasks include things like coordinating services to help prevent abuse or neglect and providing services to families who need help protecting and caring for children. They are also responsible for investigating reports of potential abuse and/or neglect, and then determining if alternative placement of children is necessary. They are also in charge of various other aspects including support services to children, achieving reunification, and more. Child protective service workers and foster care workers are the more specific workers in which these work functions are performed.
To get a good overview/understanding of what a child may experience with their family, abuse, and in the Child Welfare System (CPS and Foster Care), please follow this link and watch the two videos provided. Warning, this video may evoke some heavy emotions of sadness, so prepare yourself to watch this video: Removed Film (https://www.removedfilm.com/pages/watch)

Abused children often suffer from trauma throughout their adult lives. Patients that were exposed to trauma in early childhood can express their anxieties through drawings.
Children involved in the Child Welfare System have often experienced trauma. Trauma is defined by the National Child Traumatic Stress Network as frightening events that are overwhelming to anyone who experiences them (NTCSN, 2017). Often a person feels that their safety is a concern and is on high alert to anticipate what may or may not happen next. There are three diverse types of traumas: acute, chronic, and complex.
Before defining several types of traumas, one must understand that all types of traumas impact the brain. The stress hormone cortisol is released, then creating the fight or flight mentality. These reactions can occur any time after a traumatic experience. The link provided is a video that explains the effects of trauma on the brain and provides many explanations of how one can help others who have experienced trauma: www.changingmindsnow.org.
Acute Trauma is a single traumatic incident. An example would be a car accident or even a natural disaster. It may only be a single incident, but it can have lasting effects such as fear of being in a vehicle. Chronic Trauma is a traumatic experience that is repeated over a period. This type of trauma would include domestic violence, and war. Both have lasting effects on many people and the consequences can be hard to overcome.
Complex Trauma is a repeated traumatic experience that has been inflicted by a caregiver. This includes, but is not limited to, physical abuse, sexual abuse, and verbal/emotional abuse (also known as psychological abuse). Complex trauma leaves a child confused and conflicted. The person who inflicted harm was supposed to be the one protecting them and keeping them safe. When that does not happen, the child is then in a predicament where they do not know who to trust. A main type of trauma that will be highlighted in this chapter is complex trauma. This type of trauma occurs in various forms of abuse which are defined below.
Abuse comes in many forms including physical, emotional/verbal, and sexual abuse. According to the National Child Traumatic Stress Network (NCTSN, 2017) physical abuse is defined as any act, completed, or attempted, that physically hurts or injures a child. NCTSN also describes that act of physical abuse includes hitting, kicking, scratching, pulling hair, and more. Child Protection Services typically get reports of bruises, and other noticeable marks when investigating a report of physical abuse.
Emotional abuse is a nonphysical maltreatment of a child through verbal language. NSPCC (National Society for the Prevention of Cruelty to Children) states that emotional abuse includes “humiliation, threatening, ignoring, manipulating, and more.” (https://www.nspcc.org.uk/preventing-abuse/child-abuse-and-neglect/emotional-abuse/what-is-emotional-abuse/) Emotional abuse can be combined with other forms of abuse like physical and sexual abuse. Most reports emotional abuse is harder to prove, and thus physical or sexual abuse tends to be the main cause of removal in a home.
The link provided is where these statistics were found, and more statistics are available:
https://www.cdc.gov/violenceprevention/childsexualabuse/fastfact.html
Sexual abuse has many facets when it comes to a specific definition. Overall, sexual abuse is a “type of maltreatment, violation, and exploitation that refers to the involvement of the child in sexual activity to provide sexual gratification or financial benefit to the perpetrator. It includes contact for sexual purposes, molestation, statutory rape, prostitution, pornography, exposure, incest, or other sexually exploitative activities.” (American Society for the Positive Care of Children, 2017). The person who inflicted harm will typically use force, threats, or coercion to those who cannot/do not give consent.
Abuse does not always have to be physical, sexual, or verbal assault. It can also be neglected. According to the National Society for the Prevention of Cruelty to Children (NSPCC), neglect is the failure to meet the basic needs of a child. The NSPCC website states that neglect is the most ordinary form of abuse. According to Crossen-Tower (2010) there are three categories of neglect: physical, medical, and emotional. NSPCC adds educational neglect to the list.
When working with children who have been abused, or a family who has experienced trauma, remember that building resiliency is a key factor. Resilience is defined by the American Psychological Association (APA) as having the ability to adapt when facing adversity including trauma (APA, 2017) This, in a sense, means that one can bounce back after facing trauma. However, this does not mean that there will not be any kind of consequence or negative impact because of trauma. A resilient individual will have the tools needed to move past traumatic experiences and potential future traumas.
To help children build resiliency, the APA suggests a variety of different techniques (APA, 2017). One is to help the client build connections. Finding a support person, they can be close to, and trust will help them have the ability to attach and bond appropriately. This, in turn, will also help them be able to work through the events that they have experienced. Another factor is to help them find a positive view of themselves. Trauma can often have a negative effect on the victims’ view of themselves. Building up their confidence will not only help them bounce back from present traumatic experiences but give them the confidence to be able to move past future experiences as well.
Just like a CPS worker, a Foster Care worker can come from a variety of backgrounds including social work, criminal justice, and even psychology. Within the role of a Foster Care worker, their ultimate priority is to identify and place children who cannot remain with their parents due to safety concerns. MDHHS has protocols in place which outline the duties of a foster care worker. These include home visits and various other tasks such as interviews with biological parents and schools.
Before a child is placed with a foster family, or if the child is relocating to another foster home, there are protocols that a foster care worker follows. These protocols include providing Medicaid card/records, enrolling, or insuring the children are attending school, and providing education records to the caregiver within five days of placement. If the child is attending the same school, they previously attended then a transportation plan is to be discussed. One last example of what a Foster Care worker does is discussing any revision or plans for parents or siblings to be able to visit the child. Foster Care workers are responsible for visiting a child in the foster home. In a sense, they are searching for the same things a CPS worker would, a safe place to live, ensuring that medical needs are taken care of, and safe sleeping requirements are met, and then gathering information of how the child feels about being placed in that home. They meet with the caregivers as well to discuss various aspects of the child including medical (i.e., doctor visits, dental visits etc.), education, and behaviors portrayed in the home.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association.
American Psychiatric Association. (2017). Road to resilience. Retrieved from http://www.apa.org/helpcenter/road-resilience.aspx
American Society for the Positive Care of Children (ASPCC). (2017). Child sexual abuse. Retrieved from http://americanspcc.org/child-sexual-abuse/
Baumrind, D. (1966). Effects of authoritative parental control on child behavior. Child Development, 37(4), 887-907. doi:10.2307/1126611
Bremner, J. D. (2006). Traumatic stress: Effects on the brain. Dialogues in Clinical Neuroscience, 8(4): 445-461. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3181836/
CDC (2022). Fast Facts: Preventiing Child Sexual Abuse. Retreived from https://www.cdc.gov/violenceprevention/childsexualabuse/fastfact.html
Children’s Rights. (2017). Aging out. Retrieved from http://www.childrensrights.org/newsroom/fact-sheets/aging-out/
Edwards, J. O. (2009). The many kinds of family structures in our communities. In L. Derman-Sparks & J. O. Edwards. Anti-bias: Education for children and ourselves NAEYC. Portland, ME: Stenhouse Publishers
Enrique, J., Howk, H., & Huitt, W. (2007). An overview of family development. Educational psychology interactive. Valdosta, GA: Valdosta State University. Retrieved from http://www.edpsycinteractive.org/papers/family.pdf
The ICWA Law Center (2014). Understanding the ICWA. Retrieved from http://www.icwlc.org/education-hub/understanding-the-icwa/
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397-422. https://doi.org/10.1146/annurev.psych.52.1.397
Myers, J. E. B. (2008). A short history of child protection in America. Family Law Quarterly, 42(3), 449-463. Retrieved from https://www.jstor.org/stable/pdf/25740668.pdf
National Center for Victims of Crime. (2012). Grooming dynamic. Retrieved from https://victimsofcrime.org/grooming-dynamic/#:~:text=Perpetrators%20of%20child%20sexual%20abuse,and%20breaking%20down%20their%20defenses.
National Child Traumatic Stress Network (NCTSN). (n.d). Families and trauma. Retrieved from http://www.nctsn.org/resources/topics/families-and-trauma
National Child Traumatic Stress Network (NCTSN). (2012). Addressing secondary traumatic stress among child welfare staff: A practice brief. Retrieved from http://www.nctsn.org/sites/default/files/assets/pdfs/addressing_sts_among_child_welfare_staff_practice_brief_0.pdf
National Collaborating Centre for Mental Health (UK). (2010). Antisocial personality disorder: Treatment, management, and prevention. (NICE Clinical Guidelines, No. 77). Leicester (UK): British Psychological Society. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK55333/
National Foster Parent Association. (2016). History of foster care in the United States. Retrieved from http://nfpaonline.org/page-1105741
National Society for the Prevention of Cruelty to Children. (2017). Emotional abuse: What is emotional abuse? Retrieved from https://www.nspcc.org.uk/preventing-abuse/child-abuse-and-neglect/emotional-abuse/what-is-emotional-abuse/
Robb, M. (2004). Burned out and at risk. Washington, D.C: NASW. Retrieved from http://www.naswassurance.org/pdf/PP_Burnout_Final.pdf
State of Michigan, Department of Health, and Human Services (MDHHS). (2009). The foster child. Retrieved from http://www.michigan.gov/documents/mdhhs/e63eaDHS-Pub-435_510587_7.pdf
State of Michigan, Department of Health, and Human Services (MDHHS). (2015). Foster care/adoption/adoption/juvenile justice case worker/child visit quick reference guide. Retrieved from http://www.michigan.gov/mdhhs/0,5885,7-339-71551_7199_54039—,00.html
State of Michigan, Department of Health, and Human Services (MDHHS). (2016a). Child guardianship policy manual. Retrieved from https://dhhs.michigan.gov/OLMWeb/ex/GD/Mobile/GDM/GDM%20Mobile.pdf
State of Michigan, Department of Health, and Human Services (MDHHS). (2016b). Children’s protective services manual: Removal and placement of children. Retrieved from https://dhhs.michigan.gov/OLMWEB/EX/PS/Public/PSM/715-2.pdf
State of Michigan, Department of Health, and Human Services (MDHHS). (2017a). Child protection law. Retrieved from http://www.michigan.gov/mdhhs/0,5885,7-339-73970_7701_7869-15404–,00.html
State of Michigan, Department of Health, and Human Services (MDHHS). (2017b). Centers for Disease Control and Prevention. (n.d.). Child Sexual Abuse. Retrieved from https://www.cdc.gov/violenceprevention/childsexualabuse/fastfact.html
State of Michigan, Department of Health, and Human Services (MDHHS). (2017c). Children’s protective services investigation process. Retrieved from http://www.michigan.gov/mdhhs/0,5885,7-339-73971_7119_50648_7193-159484–,00.html
State of Michigan, Department of Health, and Human Services (MDHHS). (2017d). Foster care. Retrieved from http://www.michigan.gov/mdhhs/0,5885,7-339-73971_7117—,00.html
State of Michigan Legislature. (n.d.). Probate code of 1939: Act 288. Retrieved from http://legislature.mi.gov/doc.aspx?mcl-act-288-of-1939
United States Census Bureau. (n.d.). Current population survey (CPS): Subject definitions. Retrieved from https://www.census.gov/programs-surveys/cps/technical-documentation/subject-definitions.html
9
Learning Objectives
In this chapter the student will be reviewing:
In this chapter, the student will focus on social work practice: social work with older adults. We will consider some important considerations in the study of gerontology, common health complications for the older adult, and some of the more common concerns for the geriatric social worker.
One of the fastest-growing populations that social workers provide services to is the aging population. For social workers, older adults offer unique challenges that are not present in other populations. There are many challenges that aging adults face in our society which range from medical and mental health to financial concerns. Below are some usual challenges that they face in this country that social workers will have to be familiar with.
Among the most shared challenges facing older adults are medical conditions that attack cognition. Dementia and Alzheimer’s Disease are the most common medical conditions that older adults suffer from; both directly impair cognition to various levels. Dementia is a general term for loss of memory and other mental abilities severe enough to interfere with daily life. The most common form of Dementia is Alzheimer’s disease. In 2023, there are roughly 4.7 million Americans over 65 have dementia from Alzheimer’s disease (Alzheimer’s Association, 2023). Each form of dementia has different symptoms and physical impact on the brain. Social workers will need to be versed in several types of dementia and the interventions available to best address their clients’ needs.
Along with medical conditions that impact cognition, there are also many illnesses and diseases that impact physical health. As we age, our body begins to break down over time. Our immune systems are no longer able to fight off infections and illnesses that could occur earlier in the lifespan. There are a multitude of illnesses and diseases that the elderly population are more susceptible to. All too often, physical health deterioration leads to elderly individuals to be placed in nursing facilities, as they can no longer care for themselves without medical professionals available around the clock.
Not only are older adults more prone to diseases that impact physical health and cognition, but the population has its own unique set of mental health concerns. As we age, there are also mental health concerns that are a direct result of growing older. Depression is common among the aging population due to a variety of reasons. Grief and loss are two contributing factors to elder depression. Isolation is also a contributing factor for depression. Isolation rates for older adults are high due to physical immobility and lack of transportation. Social workers working with this population must address grief, loss, and isolation with their clients to provide better mental health care.
Managing the Cost of Aging: Another major challenge of aging is the simple cost of aging. Most older adults are unemployed due to advanced age and physical health. Many live off Social Security and retirement benefits and many utilize Medicare and Medicaid for insurance. Those who live in assisted living communities or nursing facilities have a clear majority of their income allocated for their care. The cost of medications, general living expenses, and food often monopolizes the fixed income of older adults.
Caregivers can be medical professionals, family members, or everyday individuals that provide care for the aging population in the home. Caregivers often come in the form of family such as adult children taking care of their elderly parents. Caregiving can play a demanding and strenuous role.
Many caregivers are often faced with the challenges of working outside the home while still trying to provide care. However, caregivers play a key role in enabling older adults to remain in the community for as long as possible.
Assisted living facilities are small communities or facilities that provide limited assistance for older adults. Most often, elderly couples and individuals who are still in good health will reside in these forms of care. Assisted living options offer more independence for those who reside in them. Assisted living facilities often do not employ social services, for the elders who need these services, they must be sought outside of assisted living services. Larger assisted living communities may contract with outside social service agencies to provide services.
Nursing facilities provide a wide range of services for residents. All meals and domestic services are covered by staff. There are a variety of medical professionals that are employed by these facilities. They provide 24-hour medical care for those who can no longer remain in the community and need extra support than assisted living facilities provide. Many nursing facilities also provide rehabilitation services such as physical therapy, for those recovering from surgery or serious illness.
Along with nursing staff, nursing facilities employ a broad range of professions to best provide services. Social workers, dietitians, physical therapists, maintenance staff, and environmental services are just some professions outside of nursing that are employed in these types of facilities. Social workers in nursing facilities are tasked with the residents’ mental health and emotional well-being. Social workers in these facilities most commonly work with residents who are experiencing depression, anxiety, grief and loss, and dementia. Social workers often play a significant role in nursing facilities as they may also help with admissions, day-to-day activities, and discharge planning.
The aging population faces many unique challenges. Finances, health, mental health, and political considerations must all be considered when social workers provide services to the aging population. Growing older is inevitable, however, social workers can make the process smoother than those who have entered the later stages of life.
With the various and sometimes limited resources offered, social workers must know how to navigate a system to better provide for their clients. With the rising cost of health care and an ever-changing political environment, social workers are tasked with advocating and serving those in the population who may not be able to do so themselves. People of advanced age are valuable contributing members of our world and as social workers, we must stand to make a better future for all.
Alzheimer’s Association. (2023) 2023 Alzheimer’s Disease Facts and Figures. Alzheimers Dement 19(4). DOI 10.1002/alz.13016.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association.
Mullin, E. (2013, Feb 26). How to pay for nursing home costs: Medicare, Medicaid, and other resources can help minimize the cost of long-term care. U.S. News and World Report. Retrieved from https://health.usnews.com/best-nursing-homes/articles/how-to-pay-for-nursing-home-costs
National Center on Elder Abuse. (2005). Elder abuse prevalence and incidence. Washington, DC: National Center on Elder Abuse.
National Council on Aging. (2022). Get the facts on fall prevention. Retrieved from https://www.ncoa.org/article/get-the-facts-on-falls-prevention
Nursing Home Alert: Abuse and Neglect Lawsuit Resource. (2017). State Surveys. Retrieved from http://www.nursinghomealert.com/state-nursing-home-surveys
Sollitto, M. (2016). Urinary tract infections in the elderly. Retrieved from https://www.agingcare.com/articles/urinary-tract-infections-elderly-146026.htm
10
Mental health and substance misuse are both multifaceted, challenging, and dynamic areas of the human service field. As professionals in this field, social workers help to make long lasting, life altering changes in people’s lives.
While numerous books have been written about mental disorders and substance use both broadly and specifically, this chapter will seek to introduce you to current information about mental disorders and substance use in the United States. This chapter will include, among other things, a brief history of both mental health and substance use, the current terminologies, and definitions that professionals use in the field, some of the most commonly occurring disorders and/or substances that a social worker is likely to encounter in general practice, and briefly discuss the co-occurrence of mental disorders and substance use.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition- (2013), also known as the DSM- 5, is a living document created by social workers, psychologists, medical doctors and many other professions. The DSM-5 is the primary reference source social workers and other helping professions use to describe a mental disorder. In this text, just as in the DSM-5, “mental disorder” will be used as a broad term to describe several issues related to emotion, mental state, and behavior. However, this text is not enough to help people with a mental disorder. It takes a generalist approach from social workers, as well as other health professionals, to not just identify the disorder but then advocate on behalf of that person, provide supportive services, and work with the many challenges that accompany mental health disorders.
Being a generalist means that the social worker employs various methods of treatment, expertise and skills to assist the client. Examples of methods used might be a strengths-based approach where the client is encouraged to focus on and use their inherent strengths (not just physical ones) to improve other areas of their life. Social workers also focus on the person in environment. This means that social workers are aware of the impact the person has on their environment and how the environment impacts the person.
According to the Substance Abuse and Mental Health Services Administration (SAMHSA, 2021):
Looking at those numbers it is clear to see that the need to identify, de-stigmatize and help individuals living with mental disorders will impact millions of people.
There are six categories of mental disorders that this chapter will focus on as well as the variety of disorders found within those categories. These categories contain some of the most common disorders that a social worker will encounter in her or his career. This chapter also provides a brief description of the disorders as well as the estimated occurrence, or prevalence, of each one within the United States.
The selected categories are:
Historically, people suffering from a mental disorder have also suffered abuse, experimentation, torture, and even death. As you go forth as a member of the social work profession, it is imperative that you understand how long of a road it has been and how much further the profession needs to go in the ethical treatment of people with a mental disorder.
Historically, those with a mental disorder have been looked down upon, shunned, stigmatized, vilified, criminalized, or tortured. This kind of treatment has been documented as far back as the Middle Ages of Europe all the way to the mid 1900’s- United States where those with a mental disorder were placed in either hospitals or prisons.
This treatment continued up until 1963 when John F. Kennedy signed the Community Mental Health Act. President Kennedy described it as “a bold new approach” and provided federal grants to states to construct community mental health centers (CMHC), to improve the delivery of mental health services, preventions, diagnosis, and treatment to individuals who reside in the community. To be able to supply federal funding for these statewide institutions, the Medicaid Act was passed in 1965. This Act allowed community-based care facilities to charge for reimbursement of funds while excluding payments to psychiatric institutions.
The Community Mental Health Act resulted in a mass “deinstitutionalization” across the country, and by 1980 75% of the psychiatric hospital population had declined. By 2009 less than 2% of those suffering from a mental health disorder remained in institutions. Unfortunately, this resulted in some unintended consequences. For example, community-based institutions could not keep up with the mass exodus of people from the psychiatric hospitals. This was the result of several factors such as a lack of space within the inpatient and outpatient settings, a lack of funding for proper care, and a lack of funding to improve care facilities. This lack of resources has negatively impacted the care and treatment of adults, children, families, and communities across the country.
Having a mental disorder is often compared to having a physical illness (APA, 2015) and the comparison is one that professionals can often overlook. Just as there are varying degrees of physical illnesses, there are also varying degrees of mental disorders. Mental disorders can be managed in similar ways to physical ones. By maintaining medications, therapy, and problem-solving with the individual, social workers can help the person to not only stabilize, but excel in, their life. In fact, there are many successful individuals both in today’s world and throughout history, such as Vincent Van Gogh, who have found ways to cope with their mental disorders. Van Gogh had one, even two, mental disorders. Despite, or maybe because of, these challenges he was able to produce some of the most iconic and famous pieces of modern art to this date.
Being aware of the following mental disorders will allow you, as a social worker, to better understand what the person is experiencing and how to help them meet their needs in the best feasible way.
While every case is different, it is important to start thinking about some of the ways that mental disorders may present themselves. All information and statistics following are from the DSM-5 unless otherwise indicated.
Anxiety disorders are characterized by shared features like excessive fear (the emotional response to real or perceived imminent threat) and anxiety (anticipation of future threat) and other related behavioral disturbances.
Psychotic disorders are among the most serious and challenging disorders. This is because of these disorders affect an individual’s interpretation of reality which then negatively impacts the person’s ability to function in their environments. Across the spectrum of psychotic disorders there are common symptoms such as hallucinations, delusions, or behaviors that are considered socially abnormal.
A bipolar disorder can be defined as a variance in brain functioning that can cause unusual shifts in mood, energy, or activity levels. These shifts interfere with the person’s ability to carry out day-to-day tasks. These disorders can display a range of heightened emotions in the form of manic episodes (extreme ups) to depressive episodes (extreme downs) (NAMI, 2016).
Depression affects an estimated 300 million people globally and more than 15 million adults (6.7% of the population) in the United States. There are several levels of depression as well as minor levels that co- occur with other disorders or that are brought on by substance use/withdrawal.
A personality disorder is a pattern of inner experiences and behavior that deviates from the expectations of the individual’s culture, is continuous, enduring, and inflexible; it often has an onset in adolescence or early adulthood and leads to distress or impairment in the person’s life.
These types of personality disorders are often experienced by people seeking community mental health treatment and the homeless population, both areas social workers are employed. Some personality disorders that you might encounter include:
There are two main practice settings where you as the social worker are likely to encounter people with mental disorders: inpatient (hospitals, medical & psychiatric) and outpatient (mental health clinics). Though there are some similarities in goals and strategies, the differences are certainly worth noting.
Inpatient services in these settings are provided by social workers who work with individuals or groups to provide treatment in a variety of forms. The inpatient worker also works with friends, family, and employers to help the person return to their outside life. The social worker may advocate and work with other agencies to provide assistance or resources for individuals under their purview of care.
When a patient is ready to leave a psychiatric facility, the social worker may connect them to an outpatient clinic. In these settings, outpatient workers assist individuals or groups in maintaining healthy functioning in their environment through therapy or clinical activities. The social worker in this setting will conduct therapy or planning sessions, contact outside agencies, and advocate for their client’s best interests.
While many people living with a mental disorder live fulfilling lives those who have a “severe” mental disorder are considered a vulnerable population. When we refer to people or a population as vulnerable this means it is “the degree to which a population, individual or organization is unable to anticipate, cope with, resist and recover from the impacts of disasters” (WHO, 2017). This vast population overlaps with several other populations that will/have been covered in this book:
The field of mental health is not perfect. Studies can only give us so much insight into the symptoms, behaviors, predictors, prevalence, and other criteria used in identifying mental disorders. DSM-5, while a useful tool, is still scrutinized for numerous reasons. For instance, this is the fifth edition of this text meaning that things have changed in definitions and classifications across the decades. The DSM-5, unlike its four previous versions, is being treated as a “living document” and will be amended more frequently in coming years than its previous versions. With this idea of a “living document” in mind, it isimportant to ask some questions.
There are many more questions, critiques, and changes surrounding the DSM-5, therapy styles, as well as our ever-improving understanding of the brain, and we in the social work profession must be aware of them. But it is not enough to just be aware of what we do in clinical settings. We also must be cognizant of our understanding of trauma (in its many forms), of a client’s resources and of society’s perception of what a mental disorder is. These things will continue to morph throughout time, so it is important to remain vigilant and flexible regarding the many changes that occur in our field.
Legislation could have important impacts on the services that social workers and other helping professionals offer. For example, the result of the debate over our national healthcare will have a profound impact on who receives Medicaid, how much the states will receive to supplement the costs of Medicaid funding, and what types of services will be covered.
Regardless of what your decisions or thoughts are on these issues are, the social work profession must always be vigilant of who/what/where/why/when of funding. We must also be aware politically of who’s in charge, what their agenda is, and if it impacts our profession, impacts the people we serve, and if it is in line with our professional ethics.
For decades, a war has raged across the globe. The financial costs have been high, the lives impacted even higher. During this time, we have been told to “Just Say No” and many have been arrested and imprisoned for participating in this war. The enemy in this war has taken many forms and continues to persist in modern times. It is not terror, and it is not a tyrannical government. This is a war against drugs.
Discussing substance use/abuse would be incomplete without mentioning the “war on drugs” and the historical impact substances/drugs have had on our economy, population, education, law enforcement, and policy.
Made popular in 1971, President Richard Nixon declared drug abuse “public enemy number one.” This statement came along with a dedication of more federal resources towards “prevention of new addicts and the rehabilitation of those who are addicted.” This was not a new idea by any means. The drug wars may have started as early as 1860 from certain laws at local levels. After that came the first federal law, the Harrison Narcotics Tax Act, which was signed into law in 1914. Then came Prohibition that, though ultimately unsuccessful in its attempt to make alcohol illegal, was still an attempt at eliminating an object of public consumption (Thirty Years of America’s Drug War a Chronology, 2014).
This is just the tip of the iceberg as far as the historical legislation of the war on drugs. But the questionwe should ask is: Are these policies and means of “combating drugs” really working?
According to The National Center on Addiction and Substance Abuse (2017):
To be clear, this is not to say that there should not be drug laws. Rather, the suggestion here is to consider that these laws and investments are causing more harm to the victims of drug use. These laws are not designed to prevent their use or help users to rehabilitate, as Nixon originally intended all those years ago?
It is important to note that the DSM-5 does not use the term “addiction” as a classification term. Some in the helping professions believe the term “addiction” can carry a negative connotation and is a very ambiguous definition. Therefore, the phrase “substance use disorder” is used as a more neutral term by these professionals for the purposes of describing the variety of ways that this disorder can be identified.
But, as you head into the social work profession you may find often that the terms addiction, substance use, substance abuse, and dependency may be used interchangeably or be used to refer to the same thing. For example, the term “addiction” or “addict” can be seen on government websites whereas DSM-5 employs the term “substance use disorder”. These words explain the same events, symptoms, and treatments but from two different professional standpoints, the medical (government) person centered.
The goal of the DSM-5, as well as the social work profession, is to mitigate or prevent the self-imposed and social stigmas that can result from being labeled as “an addict.” By limiting harmful stereotypes and using person centered language (i.e., saying someone has a disorder rather than calling them an addict), the client may view the disorder as a manageable part of their life rather than being all of who they are. This is an important concept for social workers to be sensitive to and it is with that in mind that this chapter will use the term Substance Use/Substance Use Disorder.
Substance use disorder (SUD) is a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues using the substance despite significant substance related problems. There are four key criteria that people must meet to be considered as having a substance use disorder: impaired control, social impairment, risky use, and pharmacological criteria.
According to the DSM-V and other sources, SUDs include but are not limited to things such as:
A social worker choosing the field of substance treatment will find themselves in two primary settings: inpatient and outpatient. Like the practice settings of mental disorders, substance use clinicians can work in inpatient clinics that house people trying to alleviate themselves of their substance use as well as enhance their health, an example of this can be seen in the film 28 Days starring Sandra Bullock. These types of facilities may have individual or group counseling sessions, provide drug screens, and provide time for the individual to reflect on their situation (Davis, 2013).
Outpatient clinics are another option for practice settings. These facilities offer potential clients scheduling flexibility and are not as intensive or hands on as inpatient facilities. These types of facilities allow clients to receive services like counseling, education, medication, and support information at their own pace (AddictionCenter.com, 2017).
According to the Centers for Disease Control and Prevention (CDC) (2017), the majority of drug overdose deaths in the United States, six out of ten, in fact, involve some form of an opioid. This epidemic is rooted in the use of prescription opiates. According to CDC statistics, half of the opioid overdoses in the United States were linked to prescription pills like OxyContin, Methadone, and Vicodin (CDC, 2017).
But what happens when the person who has been using prescription opioids can no longer afford them? They turn to heroin. According to CNN reporter, Dr. Sanjay Gupta (2016), the price for heroin is almost one tenth the price per milligram than it is for a prescription. This may be one of the many reasons we see such a rise in heroin use and is often the case, death. They may also experiment with more dangerous drugs, such as fentanyl, as has been the case of the residents of Ohio (Opiate Action Team, 2017).
All people who used heroin also used at least 1 other drug. Most used at least 3 other drugs. Heroin is a highly addictive opioid drug with an elevated risk of overdose and death for users. People who are addicted to alcohol are 2 times more likely to be addicted to heroin. People who are addicted to marijuana are 3 times more likely to be addicted to heroin. People who are addicted to cocaine are fifteen times more likely to be addicted to heroin. Prescription opioid painkillers are 40 times more likely to be addicted to heroin.
This increased trend in drug use has impacted a wide range of people and demographics, many of whom were never at “serious” risk for drug abuse before, like women, people with higher incomes, and the privately insured. Statistics show that 45% of people who used heroin were also addicted to some form of opiate painkiller (CDC, 2017). Social workers are meeting clients in hospitals as they recover from overdoses, counseling those seeking rehabilitation, work with insurance companies to distribute proper funds and ensure correct coverage, as well as educating youth on the dangers of opiates.
As we can see, there is a large spectrum of substances that have different effects on the body and brain. If you choose to enter the field of substance treatment, you are bound to encounter different ways organizations or practitioners choose to treat their clients. Two main philosophies of substance treatment are Abstinence and Harm Reduction.
Some places may encourage the practice of abstinence. You may have heard this term regarding alcohol or sex because abstinence is defined as “the act or practice of restraining oneself from indulging in something” (Oxford Living Dictionaries, 2017). Some substance uses treatment programs like Alcoholics Anonymous (AA) promote this type of behavior (DualDiagnosis.org, 2017).
According to Principles of Harm Reduction (2017), harm reduction, like many practices throughout social work, has the base philosophy of meeting people “where they are at” when it comes to their substance use. When working with a person who is experiencing problem drug use the social worker acknowledges that drugs are a part of part of this world, in both positive and negative terms (i.e., medications andillegal drugs). Rather than attacking or condemning the patient’s behavior, the clinician works with the person to minimize the use as well as the harmful effects of these substances thereby reducing the overall harm that is being done.
According to DualDiagnosis.org, 30% of people who participate in harm reduction or moderation type programs will end up in an abstinence-only program. However, according to a study conducted across a 33-month period, the success rate of abstinence only programs is very low – 5.9% for females and 9% for males (Recovery: Abstinence vs. Moderation, 2017). However, there is a current trend in this area of treatment moving more toward the use of interventions with evidence of effectiveness, but information is currently limited.
Both strategies have their limitations. For example:
What other questions do you have about substance use, abuse, and recovery?
Whether you are a social worker in mental health or substance treatment, inpatient or outpatient, there is an almost guarantee that you will encounter people who have both a mental disorder and substance use disorder in your career. This is referred to as a dual diagnosis where the presence of a mental disorder occurs along with the use of a substance.
According to the National Institute on Drug Abuse (2017), people who have a substance use disorder are nearly twice as likely to also be diagnosed with either a mood or anxiety disorder. However, a mental disorder can also lead to substance use in a sort of chicken vs. egg situation. For example, let us say there is someone who has a diagnosis of depression who also uses a stimulant to try to alleviate it. Or someone has a diagnosis of alcohol use disorder and because of this use, they have developed depression. These are two potential examples of a dual diagnosis.
As you can see, it takes a discerning professional to figure out the best path of treatment, plan for change with the individual, provide support, assist in maintaining healthy coping, and a vast array of other tasks and responsibilities.
Mental disorders and substance use are more common than people would like to admit. It adversely impacts many parts of people’s lives, whether directly or indirectly.
As a social worker in these fields, your role will be to help clients through these, potentially difficult, times. You will connect their clients to local resources, advocate for best practices to achieve client goals and outcomes and offer non-judgmental support to their clients. You yourself may even be that resource that people contact for individual therapy/counseling, or group therapy/counseling.
Social workers can seek several avenues to assist their clients. As you may already be aware, social work strives to institute evidence-based practice (EBP) when dealing directly with clients. These practices may include Cognitive Behavioral Therapy, Dialectical Behavioral Therapy, or Motivational Interviewing.
Social workers must also be familiar with medications that have been prescribed for treatment and their potential benefits, drawbacks, or chance for abuse (i.e., opiates).
Social workers working in inpatient settings may also help guide their clients through the process of detox. This process can be a long, painful, arduous process for many people and the support that a caring social worker can provide is an invaluable resource.
Social workers may lead support groups. These are organizations, outpatient, where clients gather to share their stories, successes, setbacks, hopes, and needs as they recover or maintain their mental or physical health regarding their disorder or substance use.
Finally, it behooves the social worker to know the person they are assisting. Establishing rapport, trust, and familiarity with the client’s personality, lifestyle, family structure, culture, and environment are invaluable pieces of information. The impact that a mental disorder or substance use disorder can have on these different systems are not isolated from one; these systems impact each other.
For example, someone experiencing a substance use disorder may withdraw from work or family functions seeking out isolation. They may make friends with similar substance use disorders, thereby creating a new environment that encourages behavior. The person then may not have the support to seek positive change when they decide to finally pursue help.
Similarly, someone who is diagnosed as paranoid schizophrenic may not be able to function in their working environment. This lack of employment may impact their social circles and places of enjoyment, even where they now shop. This change in lifestyle may, in turn, impact family dynamics. The family, once a great support, may now be uninformed, resentful, or frightened of the sudden change in their loved one. The rejection of family may then have an impact on the belief in oneself to recover, cope and maintain their mental health.
The area of social work that specifically deals with mental disorders and/or substance use has been around for decades and shows no signs of slowing down. In 2021 the number of social workers employed in the mental health and substance use fields was 119, 800. The field is projected to add 13,300 jobs over the next 10 years, resulting in 11% job growth (U.S. Department of Labor, 2023).
Unfortunately, the Bureau of Labor Statistics (2023) also indicates that the social workers in the mental health and substance use fields tend to make less than their peers. Workers in mental health and substance use can expect to make an average of $49,130 compared to the top average pay of $61,190 from fields like private clinical or veterans administration workers. (NOTE: Payment tends to be degree dependent; those with BSW degrees tend to make less than those with MSWs.)
Social workers have, and will continue to, advocate for the understanding of and pursuit of social justice for some of the most misunderstood and vulnerable among us. These workers will encounter a variety of individual and co-occurring disorders in their profession.
Social workers in the mental health and substance use fields continue to improve treatment outcomes with a better understanding of the brain, trauma, and evidence-based practice (EBP) models to provide treatment and care. These treatments can be in a variety of settings from community mental health (CMH) facilities, to hospitals, to private clinics.
There are many challenges in the country, as well as the world, and social workers are well equipped to combat many of these challenges going forward. This field will continue to grow over the next decade although the funding and pay scale for services is currently in question.
AddictionCenter.com. (2017). Outpatient drug rehab. Retrieved from https://www.addictioncenter.com/treatment/outpatient-rehab/
American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, DC: American Psychiatric Association.
American Psychiatric Association (APA). (2015, November). What is mental illness? Retrieved from https://www.psychiatry.org/patients-families/what-is-mental-illness
Anxiety and Depression Association of America (ADAA). (2016, August). Facts and statistics. (2016). Retrieved from https://adaa.org/about-adaa/press-room/facts-statistics
Bureau of Justice Statistics. (2017). Drugs and Crime Facts Retrieved from https://www.bjs.gov/content/dcf/enforce.cfm
Centers for Disease Control and Prevention (CDC). (2017, August 1). Prescription opioid overdose data. Retrieved from https://www.cdc.gov/drugoverdose/data/overdose.html
Davis, J. F. (2013, July 24). Day-to-day life during inpatient drug rehab. Addictionblog.org. Retrieved from http://drug.addictionblog.org/day-to-day-life-during-inpatient-drug-rehab/
Dictionary.com. (2017). Retrieved from http://www.dictionary.com/
DualDiagnosis.org. (2017). Recovery: Abstinence vs. moderation. Retrieved from http://www.dualdiagnosis.org/drug-addiction/recovery-abstinence-vs-moderation/
Gupta, S. (2016, June 2). Unintended consequences: Why painkiller addicts turn to heroin. CNN. Retrieved from http://www.cnn.com/2014/08/29/health/gupta-unintended-consequences/index.html
Harm Reduction Coalition. (n.d.). Principles of harm reduction. Retrieved from https://harmreduction.org/about-us/principles-of-harm-reduction/
Hasin, D. S., Saha, T. D., Kerridge, B. T., Goldstein, R. B., Chou, S. P., Zhang, H., …Grant, B. F. (2015, December). Prevalence of marijuana use disorders in the United States between 2001-2002 and 2012- 2013. JAMA Psychiatry, 72(12), 1-19. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5037576/
Martin, M. E. (2018). Introduction to human services through the eyes of practice settings (4th ed.). New York: Pearson.
National Alliance on Mental Illness (NAMI). (n.d.). Schizoaffective disorder. Retrieved from https://www.nami.org/Learn-More/Mental-Health-Conditions/Schizoaffective-Disorder
National Alliance on Mental Illness (NAMI). (2017). Mental health by the numbers. Retrieved from https://www.nami.org/Learn-More/Mental-Health-By-the-Numbers
National Institute on Mental Health (NAMI). (2016, April). Bipolar disorder. Retrieved from https://www.nimh.nih.gov/health/topics/bipolar-disorder/index.shtml
National Institute on Drug Abuse. (2017, February). Inhalants. Retrieved from https://www.drugabuse.gov/publications/drugfacts/inhalants
NIDA. 2021, June 1. Fentanyl DrugFacts. (2022, August 15). Retrieved from https://nida.nih.gov/publications/drugfacts/fentanyl
Oxford University Press. (2017). Oxford living dictionaries. Retrieved from https://en.oxforddictionaries.com/
PBS.org. (2014). Thirty years of America’s drug war: A chronology. Frontline. Retrieved from http://www.pbs.org/wgbh/pages/frontline/shows/drugs/cron/
Substance Abuse and Mental Health Services Administration (SAMHSA). (2015, October 27). Mental and substance use disorders. Retrieved from https://www.samhsa.gov/disorders/substance-use
United States Department of Labor, Bureau of Labor Statistics. (2017). Social Workers. Occupational outlook handbook, 2016-17. Retrieved from https://www.bls.gov/ooh/community-and-social- service/social-workers.htm
The White House, Press Office. (2017, May 23). President Trump’s first budget commits significant resources to fight the opioid epidemic [Press release]. Retrieved from https://trumpwhitehouse.archives.gov/opioids/
Wisner, B. & Adams, J. (Eds.). Environmental health in emergencies and disasters: A practical guide. Geneva, Switzerland: World Health Organization (WHO), 2002. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/42561/9241545410_eng.pdf?sequence=1&isAllowed=y
Wolf, P. (2001). Creativity and chronic disease Vincent Van Gogh (1853 – 1890). Western Journal of Medicine, 175(5), 347-348. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1071623/pdf/wjm17500348.pdf
World Health Organization (WHO). (2017). Substance abuse. Retrieved from http://www.who.int/topics/substance_abuse/en/
11
Medical social work can be defined as a specific form of specialized medical and public health care that focuses on the relationship between disease and human maladjustment (NASW, 2012; Gehlert, 2011). Medical social work is viewed as one of the most significant fields in practice. It has been acknowledged as the first subspecialty discipline to practice in hospital, public health, and clinical settings (Allen & Spitzer, 2016).
Medical social workers practice in a variety of healthcare settings such as hospitals, community clinics, preventative public health programs, acute care, hospice, and out-patient medical centers that focus on specialized treatments or populations. These professionals help patients and their families through life-changing and sometimes traumatic medical experiences. They often monitor and evaluate a patient’s mental and emotional health as they transition through a variety of medical treatments. Medical social workers also often find themselves helping the patient and family solve problems be that of financial difficulties or one-to-one counseling to help cope with new stressors (Mizrahi & Davis, 2008; NASW, 2016).
In the 20th century, social service departments in hospitals were developed to address problems associated with the increase of immigration and poverty. The need for medical social work in the United States has intensified due to the substantial inequality of health care resources. Individuals and families that live in poverty or who are a part of certain ethnic communities are additionally at a disadvantage because they are more prone to experience higher rates of acute or chronic illnesses. Therefore, the unequal distribution of healthcare insurance coverage in the United States hinders some people from seeking medical treatments due to their socioeconomic status. In 2020, 31.6 million people were uninsured in the US, including 3. million children (Cha & Cohen, 2022).
All medical social workers must familiarize themselves with cross-cultural knowledge in order to provide effective health care. They do this by familiarizing themselves with an array of different ethnicities, cultural beliefs, practices, and values that shape their family system. Medical social workers must have the ability to recognize how oppression can affect an individual’s bio-psycho-social-spiritual well-being. As future social workers, being able to understand and identify these issues will enhance your skills as a professional to provide excellent health care (Mizrahi & Davis, 2008; NASW, 2016).
The National Association of Social Workers (NASW) Standard for Social Work Practice in Health Care Setting (2016) describes eight standards of practice for health care social workers to follow. The eight goals were created as a guideline so that medical social workers would deliver excellent care. The Eight Standards of Practice for Health Care Social Workers are:
The first and second standards of practice are extremely important to remember as you become professional social workers. Social work’s primary goal is to provide excellent service and to promote social justice for all patients, thereby ensuring that all medical and psychological services are met. Therefore, all medical social workers must practice in accordance with the social work code of ethics and core values.
Medical social workers must also embrace the importance of human relationships by building a positive and lasting rapport with clients. Medical social workers advocate for the patient’s right to self-determination. Every patient is entitled to make their own decision based on treatment recommendations. The treatment team may desire and advocate for the best medical care for their patient; however, it is the patient’s decision to follow through with treatment. There are times when a patient may not be able to speak for themselves. You could encounter these situations when the patient is a child or if an adult has a cognitive impairment that enables them to make decisions for themselves. In these cases, the family has the authority to make the decision based on what they feel is the best course of action (NASW, 2016). Finally, social workers should always strive for professional competence by increasing the use of education and research and applying them to practice (NASW, 2016).
The use of multidisciplinary teams is an effective part of healthcare treatment. A multidisciplinary team is defined as a group of professionals that specialize in different disciplines that come together to deliver quality health care that addresses the patient’s well-being (Mitchell, Tieman & Shelby-James, 2008; Nancarrow et al., 2013; Allen & Spitzer, 2015). Medical social workers, physicians, nurses, and activity therapists experience several types of interactions with patients in which different behaviors are assessed, and the team then collaborates to resolve a variety of issues (Allen & Spitzer, 2015). Using this approach allows the team to provide better-quality outcomes and to enhance client satisfaction. Of course, a team may be comprised of members from the same disciplinary background. An example would be a team of medical social workers who discuss treatment plans according to the results of a patient’s assessment. Working in a team allows for individual ideas to be heard and as a group develop a specific treatment plan.
The recommended health care approach to psychological evaluations is through the use of a biopsychosocial-spiritual assessment (NASW, 2016; Social Work Licensure Exam, 2008). This approach focuses on the individual as a whole and takes into account their biological, psychological, social, and spiritual sense of self. Together the interdisciplinary team can focus on the individual’s treatment from all professional perspectives. Using this approach allows for each discipline to provide optimal health care (Gehlert & Browne, 2011).
The term biopsychosocial assessment or biopsychosocial-spiritual assessment is an approach you will hear throughout school. This model examines not just the medical aspect of care whose primary focus is on the biological causes of a disease. Rather, the biopsychosocial-spiritual model examines a patient’s well-being through a holistic approach (Gehlert & Browne, 2011; McDaniel, Hepworth & Doherty, 2014. Allen & Spitzer, 2015). The Biopsychosocial Spiritual (BPSS) Assessment offers a historical context for what the client presents with and assesses the client’s history, strengths, and resources. How do the following four areas contribute to the client’s current functioning?
The Biopsychosocial assessment may use the ROPES method of identifying strengths: Resources, Options, Possibilities, Exceptions, and Solutions (Social Work Licensure Exam, 2009).
According to The Social Workers in Hospitals and Medical Centers Occupation Profile (2017), medical social workers employ a myriad of skills and approaches to ensure quality health care. The following list provides examples of tasks that most medical social workers use when providing services.
Emergency room social workers provide services to triage patients. Depending on the location and clientele of the specific hospital, one of their main functions may be to diagnose and assess patients who show signs of mental illness. The medical social worker also performs discharge planning as a means of assurance that every patient will have a safety plan when discharged from the hospital (Fusenig, 2012). The following is a list of tasks that emergency room social workers may perform:
Hospice social workers work in a variety of different medical settings. At times, there are hospice organizations that come into a hospital to provide assistance to those who are nearing the end of their life. The following is a list of tasks that hospice and palliative care social workers perform:
One of the most important roles of all social workers is to advocate for their clients. In the healthcare system, social workers do this by representing, promoting change, speaking on behalf of the client, assessing rights and benefits, and securing social justice. It is pertinent that all receive fair and equitable access to all medical services and benefits (NASW, 2012).
The healthcare system is driven by policies that outline the rules and regulations of the organization. Policies are developed based off the organization’s ideas of acceptable and well-defined standards of healthcare practices. These policies are also implemented to reduce chaos, confusion, and legal issues that may arise due to unethical practice. Some of these policies include:
All physicians, nurses, social workers, administrative staff, and patient care workers must abide by all policies to produce effective outcomes for the organization.
Medical social workers play a very important role in the care and needs of all patients in the health care system. Above was a brief introduction to several types of medical social work job descriptions.
Always keep in mind, as you pursue your education in social work, and later in the health care field, the profession and practice will always be founded on the code of ethics.
As mentioned in Emergency Room Social Work, it may be common to identify and serve the needs of people experiencing intimate partner violence (IPV) and human trafficking, especially sex trafficking. Therefore, the following sections will introduce you to these critical areas of need.
“Violence sprouts in intimacy. Except for the police and army, family is the most violent social group, and a home is the most violent social space of our society. A person is most likely to be hit or killed in his/her own home by another member of the family than anywhere else or by anyone else” (Stark & Flitcraft, 1996)
Intimate partner violence has been recognized in the United States and other countries as a significant public health issue. This type of violence is universally condemned due to its heinous nature. The term,
intimate partner violence (IPV) is defined as any incident or pattern of behaviors (physical, psychological, sexual, or verbal) used by one partner to maintain power and control over the relationship. IPV is also considered to be an act of violence that takes place between intimate partners – heterosexual, cohabitating, married, same sex or dating (McGarry, Ali, & Hinchliff, 2016; Stark & Filtcraft, 1998).
Historically, in the United States, IPV has been considered an act of violence committed by men towards women. Although, this is still a societal belief, according to the National Intimate Partner and Sexual Violence Survey of 2010 – 2012, more than “1 in 4 men (28.5%) in the United States have experienced rape, physical violence and or stalking by an intimate partner in their lifetime, and 1 in 7 men (13.8%) have experienced severe physical violence by an intimate partner (e.g., hit with a fist or something hard, beaten, slammed against something at some point in their lifetime” (Achieng, 2017, p.2).
Intimate partner violence (IPV) refers to violence and abuse by a current or former romantic partner and includes the following types of violence (Breiding et al., 2015):
In many intimate partner violence cases, victims have the tendency to not disclose to medical professionals or law enforcement due to repercussions from the offender. Many victims fear retaliation, family separations, violation of confidentiality and security. In these instances, a social worker could do more harm than help the situation. As of 2002 only seven states have laws that make it mandatory to report actual or suspected victims of IPV (Hamberger, 2004). Most states have laws where reporting is an option. However, conditions apply for protecting an individual’s identity. Social workers can be put into these challenging positions because of confidentiality and following an ethical obligation. Potential positive outcomes and limitations from mandatory reporting by medical social workers include:
However, mandatory reporting could undermine a key component of IPV interventions of empowering the individual’s rights to self-disclosure (Hamberger, 2004).
Health/medical social workers focus primarily on the individual, family, and community to help reduce violence and its consequences. To reduce the occurrences of violence, social workers and community action agencies develop interventions to educate communities through public awareness using television commercials, billboards, radio broadcasts, IPV trainings, self-defense classes, and IPV screenings in hospitals (Haegerich & Dahlberg, 2011). There are four primary steps that health social workers take to insure a prevention plan.
Human trafficking is defined as the recruitment, transportation, and or harboring of a person by means of threat, force or another form of coercion, abduction, fraud, and deception. It is through the abuse of power over vulnerable individuals that perpetrators can exploit them. It is often combined with extreme violence, torture and degrading treatment that leave psychological wounds for the rest of their lives. Human and sex trafficking is a violation of human rights. It is estimated to effect more than two million victims worldwide (Ahn, Albert & et.al, 2013; Gajic-Veljanoski & Stewart, 2007).
In 2021 the National Human Trafficking Hotline identified over 16,000 likely vicitms of uman trafficking. “Human Trafficking”, “modern slavery” and “trafficking in persons” are all common terms to refer to when a trafficker exploits another by making them perform labor or sex acts.
There are two different forms of human tracking: (1) forced labor and (2) sex trafficking. The following section will focus on sex trafficking due to the increased prevalence in the United States. Additionally, this section will also focus on the roles that health social workers take to identify victims and to provide proper medical care (Gajic-Veljanoski & Stewart, 2007).
Sex trafficking is defined as a commercial sex act which is conducted by force, fraud, coercion, or in which the child or adult is made to perform sexual acts for money. A majority of victims in the United States come from countries such as east and south Asia, Latin America, Russia, and Eastern European countries (Salett, 2006). Health social workers play a vital role in the identification of victims. Below is a list of clues that social workers and other medical professionals look for when assisting patients in hospitals.
Victims tend to not disclose their issues due to fear of law enforcement, repercussions to family members and most are not aware of agencies that offer services specifically to the population.
Health social workers can also help eliminate the potential of sex trafficking by:
In health care settings, health social workers will encounter victims and survivors of domestic violence and sex trafficking. Having the knowledge of the increased prevalence of these two societal epidemics will allow social workers to identify victims, promote educational resources and to prevent the increase of violence.
This chapter examined the roles of medical social workers. Medical social work is a sophisticated and challenging practice that is conducted in multidisciplinary and fast-paced environments. Therefore, professional social workers in this field need to have a clear and concise understanding of the NASW code of ethics and how it relates to patient care. Medical social workers are in charge of advocating for diverse, sometimes vulnerable individuals and communities. Hospitals and insurance companies have become engrossed with enhancing the intake of profits. Because of that, it seems they lack the desire to enhance and develop a promising health care system that will support all populations. Medical social work is so important because it embraces the importance of teamwork, advocacy, and a true commitment to the individual’s medical and personal health care. Finally, please remember that just because you may not hear about or have knowingly been exposed to a societal epidemic (sex trafficking and intimate partner violence) does not mean it is not around you. Be a change agent who holistically supports the needs of each individual to enhance the quality of health care to the world.
Achieng, V. (2017, May 26). 15 countries where domestic violence is legal. The Clever. Retrieved from http://www.theclever.com/15-countries-where-domestic-violence-is-legal/
Ahn, R., Alpert, E. J., Purcell, G., Konstantopoulos, W. M., McGahan, A., Eckardt, M……. Burke, T. F. (2013). Human trafficking: Review of educational resources for health professionals. American Journal of Preventive Medicine, 44(3), 283-289. doi: 10.1016/j.amepre.2012.10.025.
American Psychiatric Association (APA). (2022). Diagnostic and statistical manual of mental disorders: DSM-5-TR. Washington, DC: American Psychiatric Association.
Allen, K. M., & Spitzer, W. J. (2016). Social work practice in healthcare: Advanced approaches and emerging trends. Los Angeles: SAGE.
Breiding, M. J., Basile, K. C., Smith, S. G., Black, M. C., & Mahendra, R. R. (2015). Intimate partner violence surveillance: uniform definitions and recommended data elements, Version 2.0. Atlanta (GA): National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Bureau of Labor Statistics, U.S. Department of Labor, Occupational Outlook Handbook, Social Workers, https://www.bls.gov/ooh/community-and-social-service/social-workers.htm
Cha, A., E. & Cohen, R., A., (2022) Demographic variation in health insurance coverage: United States, 2020. CDC national Center for Health Statistics (no. 169).
Clarke, T. C., Schiller, J. S., Boersma, P. (2020). Early release of selected estimates based on data from the 2019 national health interview survey. National Center for Health Statistics.
Fusenig, E. (2012, May). The role of emergency room social worker: An exploratory study. Master of Social Work Clinical Research Papers. Paper 26. Retrieved from https://sophia.stkate.edu/cgi/viewcontent.cgi?article=1026&context=msw_papers
Gajic-Veljanoski, O., & Stewart, D. E. (2007). Women trafficked into prostitution: Determinants, human rights and health needs. Transcultural Psychiatry, 44(3), 338-358.
Gehlert, S., & Browne, T. (Eds.). (2011). Handbook of health social work (2nd ed.). Hoboken, NJ: Wiley.
Haegerich, T., & Dahlberg, L. (2011). Violence as a public health risk. American Journal of Lifestyle Medicine, 5(5), 392 -406.
Hamberger, K. (2004). Domestic violence screening and intervention in medical and mental health settings. New York: Springer.
Human Trafficking Search. (2022). What is human trafficking? Retrieved from https://humantraffickingsearch.org/what-is-human-trafficking/
Keefe, R., & Jurkowski, E. T. (Eds.). (2012). Handbook for public health social work. New York: Springer.
Louie, K. (2017). Interview with Andrea S. Kido, LCSW, on pediatric and clinical social work. Online MSW Programs. Retrieved from https://www.onlinemswprograms.com/in-focus/interview-with-andrea-kido- lcsw-on-clinical-social-work.html
McDaniel, S. H., Doherty, W. J., & Hepworth, J. (2014). Medical family therapy and integrated care. Washington, DC: American Psychological Association.
McGarry, J., Ali, P., & Hinchliff, S. (2017). Older women, intimate partner violence and mental health: A consideration of the particular issues for health and healthcare practice. Journalof Clinical Nursing, 26(15-16), 2177-2191. doi:// 10.1111/jocn.13490
Mitchell, G., Tieman, J., & Shelby-James, T. (2008). Multidisciplinary care planning and teamwork in primary care. Medical Journal of Australia, 188(8 Suppl), S64-4. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/18429739
Mizrahi, T., & Davis, L. E. (2008). The encyclopedia of social work (20th ed.). New York: Oxford University Press.
Nancarrow, S. A., Booth, A., Ariss, S., Smith, T., Enderby, P., & Roots, A. (2013). Ten principles of good interdisciplinary teamwork. Human Resources for Health, 11(19), 1-11. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3662612/
National Association of Social Workers (NASW). (2012). Social workers in hospital and medical center: Occupational profile. Washington, DC: NASW. Retrieved from https://www.socialworkers.org/LinkClick.aspx?fileticket=o7o0IXW1R2w%3D&portalid=0
National Association of Social Workers. (NASW). (2016). NASW standards for social work practice in health care settings. Washington, DC: NASW. Retrieved from https://www.socialworkers.org/LinkClick.aspx?fileticket=fFnsRHX-4HE%3d&portalid=0
OnlineMPHdegree.net. (2017). Public health social work career, salary and job description in the field of public health. Retrieved from http://onlinemphdegree.net/public-health-socialworker/
Online MSW Programs. (2022). Hospice & Palliative Care Social Work: A Guide. Retrieved from https://www.onlinemswprograms.com/careers/hospice-palliative-social-work/
Polaris. (2022). 2021 data from the National Human Trafficking Hotline. Polaris Project.
Smith, S. G., Chen, J., Basile, K. C., Gilbert, L. K., Merrick, M. T., Patel, N., . . . Jain, A. (2012). The national intimate partner and sexual violence survey (NISVS): 2010-2012. Atlanta, GA: National Center for Injury Prevention and Control of the Centers for Disease Control and Prevention.
Stark, E., & Filtcraft, A. (1998). Women at risk: Domestic violence and women’s health. Criminal Behavior and Mental Health, 8(3), 232-234.
SAMHSA. (2021). Key substance use and mental health indicators in the United States: Results from the 2020 National Survey on Drug Use and Health. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/
SAMHSA. (2022). 2020 National Survey on Drug Use and Health Detailed Tables. US Department of Health & Human services. https://www.samhsa.gov/data/report/2020-nsduh-detailed-tables
United States Department of Health and Social Services (DHHS). (2003). Summary of HIPAA privacy rule. Retrieved from https://www.hhs.gov/sites/default/files/privacysummary.pdf
United States Department of Health and Social Services (DHHS). (2012, May). Principles of epidemiology in public health practice (3rd ed.). (Self-Study Course, SS1978). Retrieved from https://www.cdc.gov/ophss/csels/dsepd/ss1978/ss1978.pdf
United States Department of State. (2022). 2022 Trafficking in persons report. Retrieved from https://www.state.gov/reports/2022-trafficking-in-persons-report/
12
Learning Objectives
In this chapter the student will be reviewing:
Using respectful language is one of the easiest things social workers can do to build rapport with clients and help create a safer environment for services. It’s also an area that takes work! Language is constantly evolving, and throughout your career as a social worker, you will need to keep up to date with the current, best language to use with a variety of clients. When it comes to your clients with disabilities, there are several language choices to consider. Often people use a lot of euphemisms to refer to disabilities. Euphemisms are words that are substituted into conversations because they are supposedly less harsh or unpleasant. Common euphemisms for disabilities are “special needs,” “differently abled,” and “challenges.” For the most part, advocates with disabilities recommend using the term “disability” rather than any of these euphemisms. After all, “disability” is not a bad word. But even for those who use the term “disability,” there are a couple different options to choose from.
For a long time, the gold standard in the disability field was person first language. As the name implies, a person’s first language emphasizes the personhood of the individual you are talking about and suggests that disability is just one part of a person’s identity (Dwyer, 2022). For example, rather than saying “a disabled person,” you would say “a person with a disability.” Instead of talking about “the Down Syndrome woman,” you would say “the woman with Down Syndrome.” For many individuals, a person’s first language is considered the most respectful choice.
Other people with disabilities prefer identity first language. These advocates stress that disability is an important and valuable part of a person’s identity, and there is nothing disrespectful or wrong about putting disability first (Dwyer, 2022). As an example, someone who was diagnosed with autism spectrum disorder may prefer to be called “autistic” rather than “a person with autism.”
So, if some people prefer identity first language and others prefer person first language, which should you use? Ultimately, the best option is to ask your client which language they prefer. People with disabilities are the experts in their lives, bodies, and experiences, and they get to make all decisions about their care, including about what language should be used to refer to them. In this chapter, we will alternate between person first and identity first language.
One other note about language—keep in mind that some disabled people may use reclaimed terms. Reclaimed terms are words that historically have been considered offensive and have been used to speaking negatively about people with a particular identity. Individuals with these identities later reclaim the terminology that has been used against them and use it proudly as a part of their identity (Popa-Wyatt, 2020). For example, some people with physical disabilities may choose to refer to themselves as “crips,” reclaiming this word that in the past was used to oppress them. If you do not have a physical disability yourself, you should be very cautious about using this terminology. It is usually not appropriate for someone without the identity in question to use a reclaimed term.
Social workers provide services to a variety of populations on a daily basis. One such population is people with disabilities. Disabilities can take many forms, such as physical, cognitive, or mental illness (Centers for Disease Control and Prevention, 2016). The broad range of potential disabilities can pose many unique challenges for social workers. It is also important to note that while disabilities can be a singular occurrence for some individuals, disabilities often span across many population segments. In fact, about one in four adults in the United States (26%) have some type of disability (Centers for Disease Control and Prevention, 2020). It is common for people with disabilities to suffer from victimization, stigmatization, and segregation in our society. Therefore, all social workers, no matter what area of social work they are in, should be knowledgeable about the types of disabilities and those who live their lives with them. They must also be able to recognize and address ableism as it arises in their practice.
Below is a video for students to understand social work and disabilities:
There are many different types of disabilities. Sometimes it will be immediately apparent that your client has a disability, and other times they may have what is called an “invisible” or “hidden” disability. These are disabilities that you cannot see just by looking at someone. In fact, you may work with a client and never know that they have a disability diagnosis, so it is important to try to be as accessible as possible in all the work you do. Below is a description of six common types of disabilities: physical, cognitive, mental illness, visual, auditory, and speech. Keep in mind that some clients may also have multiple types of disabilities.

Physical Disability: a limitation on a person’s physical functioning, mobility, dexterity, or stamina. Physical disabilities can take many forms and can occur at any time in an individual’s life. Many physical abnormalities can occur before a person is born, developing in utero. Known as congenital disorders, these impairments can take many forms. Some can be as minor as a birth mark or as severe as a missing limb or internal abnormalities (Nemours, 2017). Sometimes congenital disabilities are referred to as birth defects, but that term is often considered offensive and outdated, so the appropriate description is congenital disability. When a congenital disability proves to be severe and long lasting, it has the potential to develop into a lifelong disability. Infants born with missing limbs or improperly developed physical traits will often grow to have a physical disability. Some physical congenital disabilities can be corrected or improved with medical technology, such as surgeries to correct cleft palates; however, there are many that cannot be corrected, potentially leading to a physical disability.
There are also physical disabilities that occur after birth at any time in an individual’s life. Major accidents are the most common cause of physical disabilities after birth. Car accidents are common accidents that can cause physical disabilities at any time in life. Car accidents can lead to minor injuries, but in severe cases can cause lifelong physical disabilities such as severed limbs, brain, and spinal cord injuries (Disabled World, 2015).
Military personnel are also at substantial risk of procuring physical disabilities through outside means. War can lead to various physical disabilities due to military engagements. The most recent military conflicts have led to high numbers of physical disabilities resulting from IEDs (Intermittent Explosive Devices) which have caused loss of limbs, spinal cord injuries and traumatic brain injuries.
Physical disabilities can impact individuals in a variety of ways. Depending on the nature of the physical impairment individuals may be limited to where they can travel, and the type of employment they can procure. Social workers must be prepared to not only address the physical limitations that a physical disability can pose, but also the emotional impact that one may have on a client. Working with clients who have a physical disability can be a unique and rewarding experience. Each client will require an individualized approach, as not everyone who has a physical disability will cope in a uniformed way.
Cognitive disabilities, also known as intellectual disabilities, are other forms of disabilities that social workers will encounter in the field. There are many types of cognitive disabilities that can vary in impact, but all affect a person’s mental functioning and skills to some extent.
Some common types of cognitive disabilities are:
Cognitive disabilities, like physical disabilities, can be present at birth. Any disability that develops before someone reaches the age of 22 is also called a “developmental disability.” Some cognitive disabilities at birth can be almost impossible to distinguish and usually begin to be present in early childhood. Some indicators of cognitive disabilities can be present in infancy, such as the infant failing to meet certain milestones or presenting unusual symptoms such as lack of sleep and inconsolable crying. While these indicators can be present, it is often difficult for medical professionals to diagnose cognitive disabilities in infants and toddlers.
Most cognitive disabilities are diagnosed in childhood and early adolescence. There are several assessments that can be conducted to determine the presence of a cognitive disability. While many medical professionals may suspect a cognitive disability, most often patients are referred out to have the appropriate assessments completed. Once a diagnosis is made there are several forms of therapy that can be performed depending on the type of cognitive disability, and early intervention at young ages can be hugely beneficial.
Even with the advancements in medical technology, there are no “cures” for cognitive disabilities. While various therapies and some medications can help improve cognition and stall deterioration in some, there is no way to fully heal the cognitive disability. Professionals can, however, make many adaptations and accommodations to provide the most accessible services possible to people with these disabilities. Cognitive disabilities can impact individuals on many levels, from employment to personal relationships. With the proper support, people with cognitive disabilities can work, live, and play in their communities. Social workers working with this population must be prepared for the diversity within and the individual challenges faced by those with cognitive disabilities.
The chapter began with a discussion of respectful language, and there are some terms used with people with cognitive disabilities that are worth unpacking. When working with clients with cognitive disabilities, you should avoid using mental age theory. Mental age theory is when someone refers to an adult with a cognitive disability as having the mind of a child (Smith, 2017). It might sound something like, “She is 25, but has the mind of a 5-year-old.” Self-advocates with intellectual disabilities have spoken against this language, explaining that it is disrespectful and hurtful to them. If you find yourself wanting to use this language, take a minute to reflect on what it is you are trying to communicate. What do you mean when you say someone has the mind of a 5-year-old? How could you communicate what you are trying to say differently? For example, you might say something like, “She is 25, but uses pictures to communicate,” or “She is 25, and needs you to talk to her in short sentences of no more than a few words.” Likely there are many other ways you can communicate valuable information about your client without using language that is disrespectful. Never treat adult clients with cognitive disabilities like they are children.
Mental Illness is considered a wide range of mental health conditions — disorders that affect mood, thinking and behavior. (Merriam-Webster’s collegiate dictionary, 1999)
While many may not consider mental illness to be a category of disability, there are several mental illnesses that impact an individual’s life in such a way that it can be classified as a disability. Mental illnesses such as Schizophrenia, Borderline Personality Disorder, and bipolar disorder can be so severe that an individual’s everyday life is impacted. When a mental illness impairs an individual’s ability to function, it can be considered a disability.
For some mental illnesses, medication can help alleviate symptoms. This is especially true regarding disorders such as Schizophrenia and Bipolar disorder. While there is no cure for these disorders, medication in combination with behavioral therapies can reduce the symptoms. However, there are some mental illnesses that even with medication and therapy can still make coping difficult.
Agoraphobia is a disorder that causes fear of places and situations that might cause panic, helplessness or embarrassment. This is one disorder that can severely impact everyday functions, to the point where the individual may not even be able to leave their home due to anxiety.
Mental illnesses in themselves can be considered disabilities when they impact an individual’s life to the point of impairing functioning. Mental illnesses can also contribute to other health concerns and behavioral symptoms that impact lives.
Individuals with visual disabilities, also sometimes called visual impairments, have a decreased ability to see, even when using glasses or contact lenses. People who are blind may have no ability to see, or very limited usable vision (American Foundation for the Blind, 2020). Visual disabilities may be congenital or can be acquired through disease or injury. Individuals who are blind or have visual impairments may use a variety of strategies to navigate through the world, such as using a guide dog or a mobility cane. Always ask before providing assistance to someone with a visual disability. Remember, they are the experts on their bodies, and they can best decide if they even need help, and if so, how they would like to be helped.
Auditory disabilities impact an individual’s ability to hear sounds, and hearing loss occurs on a spectrum. Deaf individuals have little to no functional hearing, while those who are hard of hearing have some degree of hearing loss and ability (Disabilities, Opportunities, Internetworking, and Technology, 2021). Other terms individuals in this community use are deafblind (for people with hearing and visual disabilities), deaf disabled (for people with hearing and other types of disabilities), or late-deafened (for people who become Deaf later in life) (National Deaf Center, n.d.). Many Deaf people use American Sign Language (ASL) to communicate. They may not identify as having a disability, but rather see deafness as a cultural group with its own language, traditions, and values.
Speech disabilities impact an individual’s ability to create the sounds needed to communicate with others (American Speech-Language-Hearing Association, 1993). Many speech disabilities are physical in nature, meaning the individual may have typical cognitive functioning. As you work with a client with a speech disability, you will likely learn more about their speech patterns and be better able to understand them. Never pretend to understand someone if you do not. It is better to ask a client to repeat themselves, or rephrase their statement, than to miss what they are trying to communicate.
While it is important for social workers to know about a variety of disabilities, what may be even more crucial in your practice is the ability to recognize and address ableism. Ableism is a system of discrimination based on the false belief that disabled people are inferior to nondisabled individuals. It is a form of discrimination in which disabled people are oppressed and nondisabled people are privileged (Conley & Nadler, 2022). Unfortunately, ableism is deeply ingrained in our society, and it can take many forms. One such form is physically inaccessible rooms. Think about the spaces where you spend time—your home/apartment, school, workplace, favorite coffee shop, etc. How accessible would those spaces be for someone who uses a wheelchair? Would they be able to easily enter the space, navigate through it, and exit? Surprisingly, the answer to these questions is often “no.” Social work agencies need to regularly review their spaces to ensure they are accessible for all clients, including those with disabilities.
Ableism also shows up in the form of assumptions and prejudices. For example, there is a false stereotype that people with disabilities are asexual. This false belief leads to many harmful practices, such as denying disabled people access to sexuality education (Shandra & Chowdhury, 2012). Discrimination can also cause employers to not hire people with disabilities, contributing to disproportionately high rates of unemployment among disabled people in the United States (Friedman & Rizzolo, 2017). Ableism also leads to people with disabilities experiencing higher rates of violence, such as sexual assault, than their nondisabled peers (McGilloway et al., 2018). These are just a few examples of the devastating consequences of ableism.
Below is a video for the student to understand ableism from a person with a disability perspective:
Ableism can even show up in the language we use! Sometimes, when a person rapidly changes their mind, or is acting in a way that we perceive to be overly emotional, we might say things like, “Oh, he was being so bipolar.” When we say things like this, we do not stop to think about the fact that being bipolar is someone’s actual lived experience, and it is not appropriate or respectful to use someone’s disability to insult someone else. Take a look at the list of words on the right side of the figure below. How many of these words do you use on a regular basis? If you are like most people; you use many of them a lot! Ableism is so common that it creeps into our daily conversations without our conscious awareness. We can all make efforts to use language that is less ableist. In the sections to follow, we will also talk about other ways you can address ableism in your social work practice.
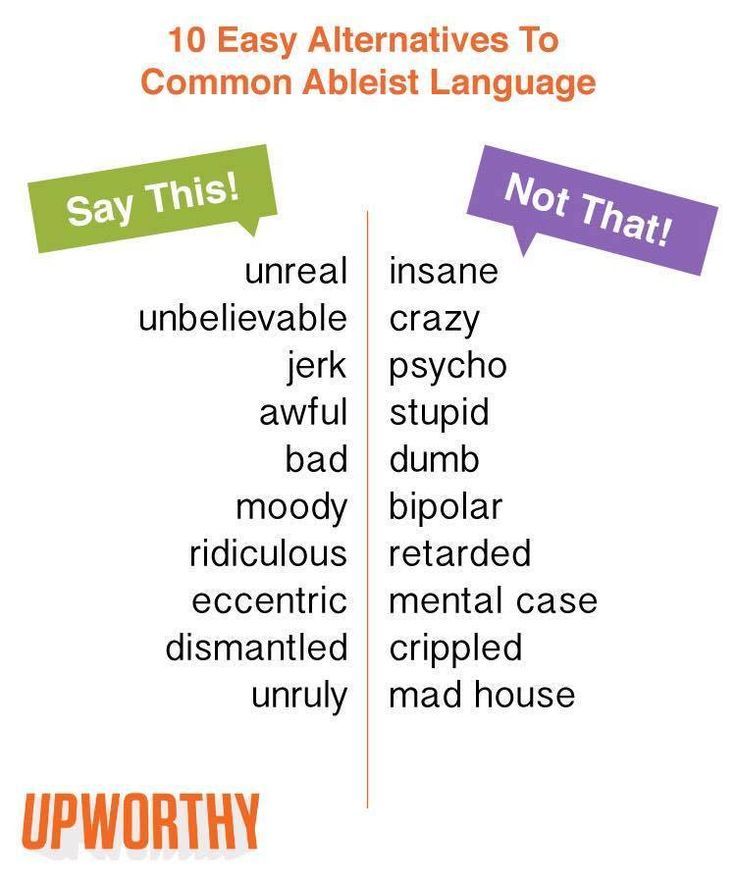
There are several models that can be used to understand disability and ableism. Three of the most common are the medical, social, and human rights models.
Under the medical model of disability, the person is understood to be disabled by their physical or cognitive condition. Individuals who subscribe to this model believe that the problem is the disability itself, and much of the focus of funding and interventions is on seeking a cure for the disability. This model puts the responsibility on the person with a disability to “overcome” the disability and adapt to the society around them. For example, if a student with dyslexia is struggling to read on grade level with her peers, the medical model would state that the problem is the student’s cognitive abilities.
The social model of disability, on the other hand, suggests that the person is disabled not by their body or mind, but by the inaccessible world our society has created. Advocates who use this model explain that we need to make accommodations to our environments and services, so they are accessible for disabled people. Disability is seen as a normal part of humanity, and it is our collective responsibility to ensure that we create spaces and services for all people. Returning to our example of the student with dyslexia who is not reading on grade level, the social model of disability suggests the problem is not the student’s disability, but rather the strategies her teachers are using to teach her to read. Accommodations need to be made for her disability, so she is better able to learn.
One of the more recently developed approaches is the human rights model of disability. This model emphasizes that disability is a normal part of human diversity, and that disabled people must have the same rights as everyone else. While there are many overlaps between the social and human rights models of disabilities, the human rights model acknowledges that there are some difficult aspects of certain disabilities, such as chronic pain or shorter life expectancy, that will still exist even after societal barriers are removed. This model suggests that individuals should also receive support for these parts of their disability that cannot be addressed through environmental and service accommodations alone (Disability Advocacy Resource Unit, n.d.). Even after the student with dyslexia receives education tailored to her needs, it still may take her extra time to read or to “catch up” to her peers, and she may be frustrated by this process. The human rights model says that we need to advocate for her rights to be treated with respect and care as she reads in the way that works best for her.
Social workers tend to follow the social and human rights models of disabilities. We understand that we have a responsibility to provide accessible services to our clients with disabilities, and to ensure their rights are being respected. The following video provides additional information on these disability models.
Social workers not only have an ethical responsibility to serve individuals with disabilities, but also a legal one. The Americans with Disabilities Act (ADA) was put into place in 1990. It guarantees equal rights for those with disabilities in the United States. It prohibits discrimination against those with disabilities “in all areas of public life, including jobs, schools, transportation, and all public and private places that are open to the general public” (ADA National Network, 2017). The purpose of the ADA is to allow the same opportunities and rights to those with a disability as everyone else. While this policy has created great advancements for those with disabilities, especially in education and employment, discrimination still takes place daily in our country.
Not everyone with a physical, cognitive, or mental health disability is limited in the same ways and the world has developed to allow more access for those with a physical disability. The Americans with Disabilities Act has helped individuals with disabilities not only because it prohibits discrimination in all areas of public life, but it has also opened many opportunities for individuals with disabilities to gain independence.
One responsibility all social workers have under the ADA is to provide reasonable accommodations for their clients with disabilities. Accommodation allows someone to do something they would not otherwise be able to do, or it makes it easier for them to do these things. All of us have used accommodations at some point in our lives. Perhaps you use spell check before turning in your homework. Or maybe you use a pill box to separate your pills by the day of the week to ensure you are taking your medication properly. Both things are accommodations! There are many different types of accommodations, but we will go over a few common ones here.
This list of accommodations only barely scratches the surface of the many different types of accommodations you can make for clients in your practice. More often than not, accommodations are simple and low-cost. You do not need to know every possible accommodation that exists—that would be impossible! What’s most important to remember is that the disabled client is the expert in their experience. They know their body and mind best, and they can tell you what accommodations would be most helpful. Allow the client to determine what kind of accommodation you provide.
Sometimes, you may also have to advocate with and for your client for an accommodation. For example, you might ask if your agency has money in its budget for ASL interpretation. If not, why not? Or perhaps your agency does not typically allow someone to have a support person present during services, but your client needs their personal care attendant present to access your services. Part of disability allyship is being willing to advocate for your client on micro, mezzo, and macro levels. This is important for social justice reasons, but also because we are all likely to experience temporary or permanent disability at some point in our lifetimes, either due to an accident or the effects of aging (World Health Organization, 2011). Designing accessible services and environments is beneficial for all.
People with disabilities face challenges in modern society that other population segments do not experience. With the various and sometimes limited resources offered, social workers must know how to navigate a system to better provide for their clients. With the rising cost of healthcare and an ever-changing political environment, social workers are tasked with advocating and serving those in the population who may need additional services navigating around the less than accessible parts of the world we live in. People with disabilities are valuable contributing members of our world and as social workers we must stand to make a better future for all.
ADA National Network. (2017). What is the Americans with Disabilities Act (ADA)? Retrieved from https://adata.org/learn-about-ada
American Foundation for the Blind. (2020, October). Key definitions of statistical terms. https://www.afb.org/research-and-initiatives/statistics/key-definitions-statistical-terms
American Speech-Language-Hearing Association. (1993). Definitions of communication disorders and variations. https://www.asha.org/policy/rp1993-00208/
Centers for Disease Control and Prevention (CDC). (2016). Disability overview: Impairments, activity limitations, and participation restrictions. Retrieved from https://www.cdc.gov/ncbddd/disabilityandhealth/disability.html
Centers for Disease Control and Prevention (CDC). (2020, September 16). Disability impacts all of us. https://www.cdc.gov/ncbddd/disabilityandhealth/infographic-disability-impacts-all.html#:~:text=61%20million%20adults%20in%20the,is%20highest%20in%20the%20South.
Conley, K. T., & Nadler, D. R. (2022). Reducing Ableism and the Social Exclusion of People With Disabilities: Positive Impacts of Openness and Education. Psi Chi Journal of Psychological Research, 27(1), 21–32. https://doi-org.ezproxy.uta.edu/10.24839/2325-7342.JN27.1.21
Disabilities, Opportunities, Internetworking, and Technology. (2021, April 9). How are the terms deaf, deafened, hard of hearing, and hearing impaired typically used? https://www.washington.edu/doit/how-are-terms-deaf-deafened-hard-hearing-and-hearing-impaired-typically-used
Disability Advocacy Resource Unit. (n.d.). How does the human rights model differ from the social model? https://www.daru.org.au/how-we-talk-about-disability-matters/how-does-the-human-rights-model-differ-from-the-social-model
Disabled World. (2015). Accidents and disability information: Conditions and statistics. Retrieved from https://www.disabled-world.com/disability/accidents/
Dwyer, P. M. A. (2022). Stigma, incommensurability, or both? Pathology-first, person-first, and identity-first language and the challenges of discourse in divided autism communities. Journal of Developmental & Behavioral Pediatrics, 43(2), 111-113. doi: 10.1097/DBP.0000000000001054
Friedman, C., & Rizzolo, M. C. (2017). “Get us real jobs:” Supported employment services for people with intellectual and developmental disabilities in Medicaid Home and Community Based Services Waivers. Journal of Vocational Rehabilitation, 46(1), 107–116. https://doi-org.ezproxy.uta.edu/10.3233/JVR-160847
Kids Health. (2017). Birth defects. Retrieved from https://kidshealth.org/en/parents/birth-defects.html
McGilloway, C., Smith, D., & Galvin, R. (2020). Barriers faced by adults with intellectual disabilities who experience sexual assault: A systematic review and meta‐synthesis. Journal of Applied Research in Intellectual Disabilities, 33(1), 51–66. https://doi-org.ezproxy.uta.edu/10.1111/jar.12445
Merriam-Webster’s collegiate dictionary (10th ed.). (1999). Springfield, MA: Merriam-Webster Incorporated.
National Deaf Center. (n.d.). Defining deaf. https://www.nationaldeafcenter.org/defining-deaf
Popa-Wyatt, M. (2020). Reclamation: Taking back control of words. grazer philosophische studien, 97(1), 159-176.
Shandra, C. L., & Chowdhury, A. R. (2012). The first sexual experience among adolescent girls with and without disabilities. Journal of Youth and Adolescence, 41, 515–532. https://doi.org/10.1007/s10964-011-9668-0
Smith, I. (2017, September 7). Mental age theory hurts people with intellectual disabilities. NOS Magazine. http://nosmag.org/mental-age-theory-hurts-people-with-intellectual-disabilities/?fbclid=IwAR3rIowvza–suPeczRKzMiw0CAKCtfQEc92vS6RyacqUD6zBAJ80rUB8Lk
Taylor, Z. W. (2018). Unreadable and underreported: Can college students comprehend how to report sexual violence? Cultivating safe college campuses conference. docs.wixstatic.com/ugd/7c1e05_885eec3ce6c1425bb4c0cd6947c7638d.pdf
Workplace Fairness. (2017). Disability discrimination. Retrieved from https://www.workplacefairness.org/disability-discrimination
World Health Organization. (2011). World Report on Disability (Rep.). Geneva, Switzerland.
13
“It seems that our relationship with our Self is most critical to all other aspects of healing work. It starts with Self and moves in concentric radiating circles out to all whom we touch.”
– Nurse Theorist and Professor Jean Watson (2005, p.133)
Before exploring the contents of this chapter about self-care, take a moment to check in with yourself. How are you? How are you feeling – physically and emotionally? What’s on your mind? Take a brief moment to answer these questions for yourself…
Now, do you have an idea of how you are and what is going with you at this moment? Great job! You have just practiced self-care! With a quick self-care practice complete, let’s take a look at self-care. What is self-care? How does one practice self-care? And why is self-care important for social work students?
As you move forward, keep in mind that self-care is a lifelong practice. Consider each section of this chapter thoughtfully, give yourself time to self-reflect as you go, and continually develop and use self-awareness to guide your experience. Self-care is not a destination; it’s a journey.
First, being a social worker and pursuing a degree in social work is demanding and, at times, stressful. Taking care of yourself, being mindful of and nurturing your health and well-being, supports academic performance and physical, mental, and emotional resilience.
There is an expression relevant to helpers, “you can’t pour from an empty cup.” Self-care is about being a healthy and vital person to serve as a model for well-being and to best help everyone for whom you will give care. In fact, according to Maslow’s Hierarchy of Needs, helping others is best accomplished when one’s own needs are being cared for.
Learning Objectives
At the end of this section, the learner will:
If you were asked to describe self-care, what would you say? Most often, people talk about the health trinity: sleep, exercise, and diet. If you think back to Maslow’s Hierarchy of Needs, those are certainly very important components of self-care. However, self-care can be so much more – an idea that is explored in more detail later in this chapter. The most useful definition of self-care may be: self-care is anything that makes you better. To explore this idea, let’s first look at self-care through the lens of the health trinity.
Sleep is an essential part of your daily routine. Sleep allows your brain to “reset” and your body to remain healthy. The sleep-wake cycle consists of roughly 8 hours of nocturnal sleep and 16 hours of daytime wakefulness. This cycle is controlled by two internal influences: sleep homeostasis and circadian rhythms. More than 25% of the U.S. population report occasionally not getting enough sleep. Nearly 10% have chronic insomnia (Centers for Disease Control & Prevention, 2009). These can be serious problems for a college student.
Sleep loss results in a “sleep debt.” Sleep debt is the accumulated loss of sleep that is lost due to poor sleep habits. Like any other debt, sleep debt must eventually get repaid, or there will be consequences to personal health and well-being. For example, staying awake all night results in a sleep debt of 7 to 9 hours. Our bodies will demand that this debt be repaid by napping or sleeping longer in later cycles. Even loss of one hour of sleep over several days can have a negative effect.
Insufficient sleep is associated with a number of chronic diseases and conditions such as diabetes, heart disease, obesity, and depression. As well, daytime sleepiness can affect mood, performance, and memory. One research study found that students who stayed up all night simulating “pulling an all-nighter” studying scored 40% lower on a general test compared to students who got the recommended amount of sleep (Walker, 2019). That means that getting a good night’s sleep can be the difference between making an A and a D on an important test.
The National Sleep Foundation recommends:
The National Sleep Foundation has many resources including sleep facts and tips for restful sleep: www.sleepfoundation.org
National Sleep Foundation, (2009)
Sleep Activity: What’s your Chronotype?
All of our bodies follow a 24-hour sleep-wake circadian rhythm. However, not everyone’s rhythm is the same. Some are more alert earlier in the day, while others come to life a bit later. This variation is known as your chronotype.
A simple way to classify chronotypes are: morning lark, day dove, and night owl. Morning larks are, naturally, early to bed and early to rise. Night owls, by contrast, get going and may have an alert and productive period later in the day. Day doves seem to fall somewhere in the middle.
Based on your answers, This might be a good time to do more important and challenging work, like writing a paper or doing more focused studying.
The importance of getting regular exercise is probably nothing new to you. The health benefits are well known and established. Regular physical activity can produce long-term health benefits by reducing your risk of many health problems, such as heart disease, cancer, and diabetes, and it can also increase your chances of living longer, help you control your weight, and even help you sleep and think better.
As a busy college student, you may be thinking, I know this, but I don’t have time! I have classes and work and a full life! What you may not know is that—precisely because you have such a demanding, possibly stressful schedule—now is the perfect time to make exercise a regular part of your life.
Getting into an effective exercise routine now will not only make it easier to build healthy habits that you can take with you into your life after college, but it can actually help you be a more successful student, too. In addition to keeping your heart healthy, helping with weight loss, and helping you live longer, regular exercise can also improve your mood and help keep depression and anxiety at bay. Exercise is a powerful tool for stress management and improving one’s mental health and memory—all of which are especially important when you’re in school.
The good news is that most people can improve their health and quality of life through a modest increase in daily activity. You don’t have to join a gym, spend a lot of money, or even do the same activity every time—just going for a walk or choosing to take the stairs (instead of the elevator) can make a difference. Studies continue to show that it’s never too late to start exercising and that even small improvements in physical fitness can significantly improve overall health.
You can be successful with the inclusion of an exercise regime in your new life, but it is very important to find an activity that you like. Setting a schedule is advisable for success in your program. Also, doing a variety of activities will result in less boredom, and incorporating fun activities with family and friends can be very encouraging. The Maverick Activities Center (MAC) offers a wide range of exercise options from free-play sports, exercise equipment, swimming, indoor track, and more. Getting involved in intramural sports can also increase your activity level while meeting some social needs. Also, you will have the opportunity to walk on campus to contribute to your exercise activity, so don’t be so concerned with finding the closest parking spot available.
In addition to formal exercise, there are many opportunities to be active throughout the day. The more you move around, the more energy you will have. The following strategies can help you increase your activity and energy levels:
Workout or Work in?
Fitness expert Paul Chek says that the best workout is the one that you will do repeatedly.
Paul Chek also has a concept of working out vs. working in. A workout is a strenuous exercise session like weightlifting, sprinting, or intense cardio. Working in, on the other hand, is doing more gentle, energy-building movement and exercise; it’s not energy depleting but energy generating. Examples of working include yoga, tai-chi, qi gong, stretching, and walking.
A diet is anything that you consume on a regular basis. If you drink Diet Coke for breakfast every day, that’s part of your diet. When people talk about “going on a diet,” they usually mean changing their existing dietary habits in order to lose weight or change their body shape. Everyone is on a diet because everyone eats!
Having a healthy diet means making food choices that contribute to short- and long-term health. It means eating the right amounts of nutrient-rich foods. The right mix can help you be healthier now and in the future. Developing healthy eating habits doesn’t require you to sign up for a gimmicky health-food diet or lifestyle; you don’t have to become vegan, gluten-free, “paleo,” or go on regular juice fasts. The simplest way to create a healthy eating style is by learning to make wise food choices that you can enjoy, one small step at a time.
College offers many temptations for students trying to create or maintain healthy eating habits. You may be on your own for the first time, and you’re free to eat whatever you want, whenever you want. You may not be in the habit of shopping or cooking for yourself yet, and, when you find yourself short on time or money, it may seem easier to fuel yourself on sugary, caffeinated drinks and meals at the nearest fast-food place. Cafeterias, all-you-can-eat dining facilities, vending machines, and easy access to food twenty-four hours a day make it tempting to choose hyper-palatable, nutrient-deficient unhealthy foods and overeat.
Ideas for healthy eating
There are a wide array of healthy foods and ways of eating. Like exercise, find the healthy foods and dietary approach that you like, that makes you feel good, and that you can naturally and easily sustain your lifestyle.
As you find what works for you, it’s important to remember that it’s common for people to overeat (or not eat enough) when they feel anxious, lonely, sad, stressed, or bored, and college students are no exception. It’s incredibly important to develop healthy ways of coping and relaxing that don’t involve reaching for food, drink, or other substances. While self-care does involve the health trinity, there are other important elements, including stress management.
Planning a Healthy Day
It’s been said that if you fail to plan, you plan to fail. Take a few minutes and write out what a full day of healthy eating looks like for you.
Use your findings as a way to begin to design a healthy eating meal plan for yourself.
Learning Objectives
At the end of this section, the learner will:
If you’re a college student, it may feel like stress is a persistent fact of life. In fact, a wide range of research from the last two decades finds that one of the top challenges to academic performance is college student stress. Scott (2009) notes that academic stress is caused by the different workload in college, challenging classes, and an independent learning structure. Freshmen face social stresses such as a new social network, less parental support, being away from home, living with a roommate, part-time jobs, and the dynamics of relationships. Other stresses include day-to-day chores, time management, and the developmental tasks of young adulthood. If not managed, stress can result in feelings of being overwhelmed, which can result in unhealthy habits like heavy drinking, weight issues, and the possibility of dropping out of college.
Sometimes stress can be good. For instance, it can help you develop skills needed to manage potentially challenging or threatening situations in life. However, stress can be harmful when it is severe enough to make you feel overwhelmed and out of control. While everyone experiences stress at times, a prolonged bout of it can affect your health and ability to cope with life. It’s not only unpleasant to live with the tension and symptoms of ongoing stress; it’s actually harmful to your body, too. Chronic stress can impair your immune system and disrupt almost all of your body’s processes, leading to increased risk of numerous health problems, including:
The potential health problems associated with stress reflect why it’s so important to learn healthy ways of coping with the stressors in your life. The best strategy for managing stress include taking care of yourself in the following ways:
If the self-care techniques listed above aren’t enough and stress is seriously interfering with your studies or life, don’t be afraid to get help. The student health center and Counseling and Psychological Services (CAPS) are both good resources.
Stress Management: What Works for You?
How might you use the stress management techniques mentioned above? For example:
Returning to our definition of self-care – self-care is anything that makes you better – there is an addition that may help direct you in further developing your approach. Humanist Psychologist Carl Rogers described the healthy and vital individual as a fully functioning person. According to Rogers, this person strives to and may act in congruence with what they envisioned as their ideal, best self. This was the process that Rogers referred to as self-actualization, and as a precondition to authentically helping others. Based on this understanding, a revised definition of self-care could be: self-care is anything that makes you better and helps you live more like your best self.
Previously mentioned was the idea that self-care says, “you can’t pour from an empty cup.” If self-care is, in part, about realizing our best selves, it matters what you fill your cup with. There may be times when getting food-to-go and watching Netflix is the best thing for your mind, body, and soul. Other times, those same things could just be more junk that isn’t serving you or your development towards your best self. Therefore, when you think about your self-care needs, it may be crucial to ask:
To help guide you in recognizing and acting in alignment with your ideal self, self-awareness and self-compassion may be essential.
My Best Self
Describe your best self. At your best, according to you:
Find a time to give yourself 20 minutes or more of uninterrupted writing.
Learning Objectives
At the end of this section, the learner will:
It’s been said that in order to grow yourself – grow towards your ideal self – you must know yourself. That’s self-awareness. Self-awareness is being consciously aware of yourself, your feelings (physical and emotional), your thoughts, motivations and drives, and your behaviors. Developing self-awareness may go by many names and take many forms.
Greater awareness of self can be accomplished through self-reflection, introspection, mindfulness, or meditation, to name a few. This is the more internally-focused form of self-awareness. Self-awareness can also be gained through feedback from other, trusted people in your life. This is a more externally-focused form of self-awareness. Both forms of knowledge about self are useful and can lead to an array of improvements in your life. To embark on a well-balanced journey of self-awareness consider the following actions:
As you explore self-awareness, you may notice that you can be tough on yourself, overly negative or critical, and begin feeling insecure. Pastor Steven Furtick said, “the reason we struggle with insecurity is because we compare our behind-the-scenes with everyone else’s highlight reel.” Not only can taking seriously the feedback of others be helpful, adopting a self-compassionate perspective can help, too.
Journaling
A great way to begin to explore and know yourself is journaling. While there are many ways to do this, the most important aspect is simply to do it. You can write on paper, type it out, or even dictate notes on your phone. You can do it in the morning to prepare for your day. Journal throughout the day as a way of checking in with yourself. Or you can journal at night to clear your head, release the stress or the day and day upcoming, and more fully relax and rest! You can write for a long time or you can simply make notes or bullets about things you want to get out of your head and onto paper.
Try journaling for a day or two. Come back to class and report how the experience was, how you did it, what worked, what didn’t, what you learned, and learn from others.
While you may be familiar with self-awareness, self-compassion may be newer to you. Kristen Neff, a leading self-compassion researcher, explains that compassion for yourself is no different for the compassion and patience you have for others. According to Neff (n.d.), compassion has three parts: (1) noticing suffering, (2) being moved by and responding to that suffering, and (3) recognizing that suffering and imperfection is something we all share in common. Therefore, self-compassion is responding to your own struggles and imperfection the way you would a good friend or loved one: with kindness.
To begin your practice in self-compassion, consider the following questions:
(Tartakovsky, 2018)
To learn more about self-compassion and for exercises to develop it, visit Self-compassion.org
Ultimately, Neff explains that “self-criticism asks: are you good enough? [while] self-compassion asks: what’s good for you?” Self-compassion seen through this lens aligns perfectly with the best self-care: self-care done your own way and always with a conscious aim to make yourself better!
Reflect and Share
Take a few minutes in class to answer the self-compassion questions above and discuss your findings with a partner, small group, or as a class.
Being a social work and school can be stressful. The healthier and more vital you are, the better your work and academic performance will be. Better yet, you can only give what you have. The healthier and more vital you are, the more health and vitality you will have to help, support, and give to others. Self-care is not selfish. Self-care is an essential foundation to most authentically helping others. As nurse theorist and professor, Jean Watson, so beautifully shares, self-care is the most important aspect of healing work. Healing, health, and vital life for all starts with you!
1
Introduction to Social Work
The History of Social Work in the United States
Ethics
Culture and Diversity
Poverty
Social Work Practice
Generalist Practice
Social Work Practice with Children and Families
Social Work with Older Adults
Mental Health and Substance Abuse
Social Work and the Health Care System
Social Work with Persons with Disabilities
2
This work contains copyrighted material the use of which has not always been specifically authorized by the copyright owners. The creators of this OER believe in good faith that reuse of these materials constitutes a “fair use” as described in Section 107 of the Copyright Act. Downstream users who wish to use copyrighted material from this resource for purposes beyond those authorized by the fair use doctrine should obtain permission from the copyright owner(s) of the original content.
Unless noted below, all figures used in the text were originally published in Introduction to Social Work at Ferris State University and are licensed under a Creative Commons Attribution 4.0 International license.
“Branch Settlement House” by University of Illinois is in the Public Domain.
“Figure 16.13” by Rose M. Spielman, William J. Jenkins, and Marilyn D. Lovett is licensed CC BY 4.0.
“Building web accessibility by considering different types of disabilities” © Apurva Shah & Alison Sizer, ESRI
“10 Easy Alternatives to Common Ableist Language” © Franchesca Leigh, chescaleigh
3
This open textbook is adapted from the textbook Introduction to Social Work at Ferris State University by the Ferris State University Department of Social Work, which is licensed CC BY 4.0. The chapter “Self-Care: Strategies for Personal and Professional Success” is adapted from the chapter of the same name in Strategies for Success in Nursing School: From Start to Finish by Leslie Jennings, RN, RaeAnna Jeffers, Laura Haygood, and Craig Keaton, which is licensed CC BY 4.0. The following index details where content was used in this manuscript. Major and minor revisions were made throughout the book.
“CHAPTER 1: INTRODUCTION TO SOCIAL WORK” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 1: INTRODUCTION TO SOCIAL WORK” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 2: NASW CODE OF ETHICS” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 3: CULTURAL COMPETENCE” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 6: POVERTY” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 5: SOCIAL WORK PRACTICE SETTINGS” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 4: GENERALIST PRACTICE” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“Solution-focused brief therapy” – Wikipedia, license CC BY-SA 3.0.
“CHAPTER 7: CHILD WELFARE AND FOSTER CARE” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 8: GERONTOLOGY AND PEOPLE WITH DISABILITIES” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 1: INTRODUCTION TO SOCIAL WORK” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 1: INTRODUCTION TO SOCIAL WORK” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“CHAPTER 8: GERONTOLOGY AND PEOPLE WITH DISABILITIES” – Introduction to Social Work at Ferris State University, licensed CC BY 4.0.
“Self-Care: Strategies for Personal and Professional Success” – Strategies for Success in Nursing School: From Start to Finish by Leslie Jennings, RN, RaeAnna Jeffers, Laura Haygood, and Craig Keaton, licensed CC BY 4.0.